What Does the Otolaryngologist Need to Know about Thyroid Radiofrequency Ablation?
Our specialty is considered a leader in the management of thyroid disease, and it is therefore natural for us to be one of the early adopters of RFA.
Antoine Eskander, MD, ScM, FRCSC, Head and Neck Surgery Education Committee Member
The adoption of new technologies in medicine is characterized by a predictable life cycle. While radiofrequency ablation (RFA) is not new technology, the early adopters in Korea published their first consensus statement on the use of RFA for the thyroid in 2012, where the technology is now commonly used and is in the late majority part of the adoption life cycle. In North America, the technology is in the early adopter stage in part due to delays in getting regulatory approval for the technology (2018 FDA and 2023 Health Canada).
While the standard of care for malignant, suspicious, and indeterminate thyroid nodules continues to be surgical resection, with a few caveats including the addition of molecular testing and active surveillance, the management of benign and autonomously functioning thyroid nodules is evolving.
The most benign appearing nodule is one that is entirely cystic. Such nodules are not well managed with RFA and can be managed with alcohol ablation with a high success rate in patients who wish to have this treatment for symptomatic or cosmetic concerns. However, alcohol ablation is not as successful in nodules that are solid cystic.
So, on whom are we currently considering thyroid RFA? The main indications include patients with the following:
- Benign thyroid nodules (typically with two separate biopsies) that are either symptomatic or leading to cosmetic concerns and
- Toxic autonomously functioning thyroid nodules.
Contraindications include:
- Nodules with ultrasound characteristics suspicious for malignancy
- Follicular neoplasm and malignant lesions on biopsy and
- Purely cystic nodules.
Other indications are being investigated but are certainly not standard of care and should only be considered in the context of a clinical trial.
Currently RFA is performed worldwide and can be performed by interventional radiologists, endocrinologists, and surgeons. The North America Society for Interventional Thyroidology (NASIT) was created to promote the safe integration of ablative thyroid technologies and includes members from all three disciplines. Comfort with advanced ultrasound techniques including thyroid ultrasounds, fine needle aspiration biopsy of thyroid nodules, and core biopsy techniques in the neck are critical.
This makes our specialty an excellent group to engage in RFA given our strong commitment to managing thyroid disorders and our growing comfort and experience with thyroid ultrasound. At the very least, our specialty should have a strong understanding of the indications, contraindications, risks, and benefits of this technology so that we can best advise our patients on all the available options in the management of their thyroid nodules.
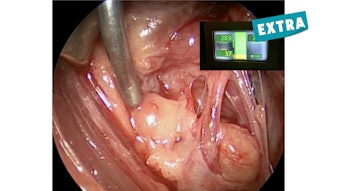
What surprised me the most about RFA as I started to incorporate it into my practice is how involved it is as a procedure. This is not as simple as an ultrasound guided biopsy. The procedure is performed with patients awake, lying supine, in the neck extended position, and with local anesthetic both locally in the skin but also with dextrose along the visceral fascia using a hydrodissection technique to protect lateral nodules from the carotid and esophagus.
The procedure can be as quick as 30 minutes for small hyperfunctioning nodules but can take as long as two hours in larger nodules. The procedure requires advanced ultrasound skills with visualization of the tip of the probe during the majority of the procedures and certainly during probe activation using a long-axis trans-isthmic approach. Unlike hepatic lesions, for thyroid nodules the moving-shot technique is used, which requires probe movement in an orderly fashion throughout the nodule. A nurse or assistant is required during the procedure for patient monitoring and to provide additional equipment while maintaining sterility.
The probe needs to avoid the danger zone, which is from the tracheoesophageal groove medially to the carotid artery laterally that encompasses the variable location of the recurrent laryngeal nerve (particularly on the right) as well as the vagus nerve. The procedure ends when all the visualized portions of the nodule appear ablated on the ultrasound. The procedure may also end if the thyroid nodule lies too close to critical structures such as the trachea, the esophagus, and the recurrent laryngeal nerve, or if the inferior aspect of the nodule is no longer visualized on the ultrasound and extends into the upper mediastinum.
While the procedure is only being performed by high volume surgeons, endocrinologist, and interventional radiologists, the technique is known to have a low but real complication rate. Voice chance is the most common major complication (1%) and is typically temporary (60-90 days). Nodule rupture may lead to abscess formation; however, this is uncommon (<0.2%). Minor complications include hematoma (1%), skin burn (<1%), and most commonly pain (2.6%).
The success rate of RFA in shrinking benign thyroid nodules is extremely high with volume reduction in the order of 60%-80% at one year. It should be noted that after RFA thyroid nodules will appear ugly or concerning on ultrasound as they are often irregular, hypoechoic, and with microcalcifications. Working with experienced ultrasonographers and indicating which nodules have been ablated are therefore critical components of the follow up of thyroid RFA patients.
Otolaryngologists have always been innovative, technologically and technically savvy surgeons, with an eagerness to provide comprehensive care for our patients. Our specialty is considered a leader in the management of thyroid disease, and it is therefore natural for us to be one of the early adopters of RFA. I would encourage members of the AAO-HNS, particularly those with a significant endocrine surgery practice, to learn more about RFA and incorporate it into your practice.