Hyper- and hypocalcemia are common problems encountered by otolaryngologists in the academic and private practice setting.
David C. Shonka, Jr., MD, and David L. Steward, MD
Hypercalcemia
When hypercalcemia is identified in the outpatient setting, it is most commonly due to primary hyperparathyroidism. The diagnosis of hyperparathyroidism is based on biochemical results. Classically, parathyroid hormone (PTH) and calcium levels are simultaneously elevated with normal (not suppressed) 24-hour urine calcium levels. Suppressed 24-hour urine calcium levels may indicate familial hypercalcemic hypocalciuria that can be confirmed with genetic testing. Low urinary calcium levels may also result from chronic renal insufficiency and diuretics, particularly hydrochlorothiazide.
There are also low-biochemical profile versions of hyperparathyroidism termed normocalcemic and normohormonal hyperparathyroidism. Normocalcemic hyperparathyroidism should be differentiated from other causes of PTH elevation. Generally, other causes of PTH elevation are secondary to calcium depletion. This can be due to chronic renal disease, inadequate dietary calcium intake, renal calcium leak, or poor calcium absorption due to Vitamin D deficiency, chronic proton pump inhibitor therapy, or prior gastric bypass. Typically patients with secondary PTH elevation will have low or low normal calcium levels.
Conversely, patients with normohormonal hyperparathyroidism should be evaluated for other possible causes of hypercalcemia. The differential diagnosis for hypercalcemia is extensive and causes may include malignancy, excessive exogenous supplementation, granulomatous disorders, and others. Lab testing can help rule out some of these other causes. Elevated PTH-related protein, serum protein electrophoresis, and 1,25-dihydroxyvitamin D levels indicate potential alternative causes of hypercalcemia such as lung cancer, multiple myeloma, and granulomatous disorders respectively. Typically PTH levels will be subnormal when hypercalcemia is due to other causes. Normal and even low normal PTH levels have been reported in patients with pathologically confirmed primary hyperparathyroidism. Interestingly these patients have a disease profile more similar to classic primary hyperparathyroidism than patients with normocalcemic hyperparathyroidism with a similar incidence of single gland disease, size of causative adenoma, and likelihood of preoperative imaging localization. In general, parathyroid surgery should be avoided in patients with hypercalcemia due to other causes.
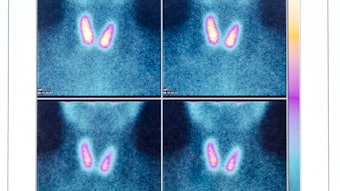
Once a diagnosis of primary hyperparathyroidism has been made and the physician and patient have agreed that surgery is indicated, imaging studies are useful for preoperative localization.1 Ultrasound is an excellent initial localization study. It is low cost, results in no radiation exposure for the patient, and is the best study for identification of coexisting thyroid pathology that may be present in up to 50% of patients. Ultrasonography is able to identify the abnormal parathyroid gland in 80%-90% of patients with single gland disease (Figure 1).
Figure 1. Intrathyroid left inferior parathyroid adenoma with polar blood flow pattern.
Parathyroid surgeons may choose to become proficient at neck ultrasonography as studies show an advantage to surgeon performed ultrasound with high sensitivity and specificity.2 Sestamibi (planar) scanning utilizes the tendency of parathyroid glands to concentrate 99mTc-sestamibi to localize abnormal glands. Single photon emission computed tomography (SPECT) produces 3D images and can be fused with a low CT to create SPECT/CT studies. Combined with delayed imaging, these have a high degree of sensitivity and specificity for parathyroid localization. Sestamibi imaging performed immediately preoperatively also allows for the use of radiolocalization intraoperatively. Limitations of this imaging modality include small glands, patients with multigland disease, and variability in quality and availability of SPECT/CT between institutions. Contrast enhanced CT has been increasingly utilized in parathyroid localization and is often referred to as four dimensional CT (4D-CT). In its simplest form, this uses non-contrast images and arterial phase contrast enhanced images to identify parathyroid adenomas. On non-contrast images, a parathyroid adenoma should appear hypodense relative to the thyroid gland. The parathyroid adenoma should avidly enhance on arterial phase contrast images (Figure 2).If a venous washout phase is included, parathyroid adenomas should have early venous washout relative to the thyroid and lymph nodes. 4D-CT is especially useful in re-operative parathyroid surgery and is good for identifying deep superior parathyroid adenomas that may not be visible on ultrasound. It has been shown to successfully identify small glands that may not be seen on other imaging modalities. Because of the contrast load, it should be avoided in patients with renal insufficiency.
Figure 2. Axial CT non-contrast (left) and arterial phase contrast (right) demonstrating left thyroid tubercle (+) and right superior parathyroid adenoma (*). The parathyroid adenoma is hypodense relative to the thyroid gland on the non-contrast image and avidly enhances on the arterial phase contrast image while the thyroid tubercle is isodense to the thyroid on the non-contrast image.
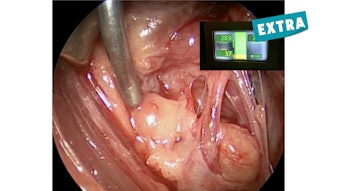
If a parathyroid adenoma is identified on preoperative imaging, a targeted approach to the involved gland may be undertaken at the time of surgery (Figure 3). When a single abnormal gland is identified and removed, intraoperative PTH monitoring is a useful adjunct to determine completeness of surgery. Varying criteria have been proposed to define an appropriate PTH reduction. A 50% reduction from a baseline pre-incision level at 10 minutes after gland removal with the final PTH in the normal range is correlated with a high likelihood of cure (normal calcium at six months postoperatively). In the absence of preoperative localization or appropriate PTH reduction after targeted adenoma removal, a four gland (bilateral) exploration should be undertaken.
Figure 3. Minimally invasive left interior parathyroidectomy. Left Inferior parathyroid adenoma (*) and left thyroid lobe (+).Hypocalcemia
Hypocalcemia is the most common complication after total or completion thyroidectomy. Permanent hypocalcemia has been reported to occur in up to 6% and temporary hypocalcemia in up to 50% of patients. The pre-, intra-, and postoperative phases all offer opportunities for management of hypocalcemia. Careful preoperative evaluation may identify patients at risk for hypocalcemia. Surgery for patients with Grave’s disease, thyroid cancer, bulky nodal disease, and planned central neck dissection in conjunction with total thyroidectomy increase the risk of hypocalcemia. Evaluation of preoperative calcium, vitamin D, and PTH levels may identify patients with secondary hyperparathyroidism who are more dependent on robust parathyroid function for maintenance of an eucalcemic state. These patients are at greater risk of postoperative hypocalcemia, particularly when sustaining parathyroid damage intraoperatively, and some patients may benefit from calcium and/or calcitriol supplementation in the days leading up to surgery.
Intraoperatively, care should be taken to preserve the parathyroid glands as well as their delicate blood supply. The parathyroid glands are often supplied by small vessels entering from their medial aspect. It is important to address the branches supplying the thyroid while preserving the parathyroid branches. Near-infrared autofluorescence is an emerging technology that may aid the surgeon in the identification and preservation of parathyroid glands during thyroid surgery.3 Parathyroid glands that are inadvertently removed or devascularized should be minced and reimplanted in a well vascularized bed of tissue. Reimplanted parathyroid tissue typically becomes biochemically active around 28 days from surgery and may help prevent permanent hypocalcemia.
Different strategies are available for postoperative calcium management. Some surgeons elect to empirically treat all patients undergoing total or completion thyroidectomy with calcium and/or vitamin D supplementation. A common approach is oral calcium carbonate plus vitamin D, 1000 mg three times daily for one week, twice daily for one week, and then once daily for one week. For patients with significant hypoparathyroidism, this may be inadequate. These patients also require calcitriol (activated vitamin D) 0.25-1.0 mcg qd - bid. Supplementation with calcium citrate should be considered in patients on proton pump inhibitor therapy as an acidic environment is necessary for absorption of calcium carbonate. An alternative approach is to use lab testing to identify patients who would benefit from calcium supplementation. Formerly this was accomplished by trending calcium levels. More recently, absolute PTH level or change in PTH levels from baseline as early as 30 minutes postoperatively has been shown to identify patients at risk of hypocalcemia.4 Permanent hypocalcemia due to hypoparathyroidism is typically managed with lifelong calcium and vitamin D supplementation. Daily parathyroid hormone subcutaneous injections appear to decrease dependency on calcium and vitamin D supplementation. This has been approved by the U.S. Food and Drug Administration (FDA) but carries the potential risk of osteosarcoma and has limited availability.
Hyper- and hypocalcemia are common problems encountered by the practicing otolaryngologist. A high degree of clinical acumen is often required to differentiate low biochemical profile versions of primary hyperparathyroidism from other causes of hypercalcemia and elevated PTH levels. Familiarity with parathyroid imaging modalities and sound surgical technique are important in successful parathyroid surgery as well as parathyroid gland preservation in thyroid surgery. As otolaryngologists continue to make advances in the diagnosis and management of these disorders, more patients will be spared the long-term detrimental impacts of hyper- and hypocalcemia.
References
Zafereo M, et al. American Head and Neck Society Endocrine Surgery Section update on parathyroid imaging for surgical candidates with primary hyperparathyroidism. Head Neck. 2019 Jul;41(7):2398-2409. doi: 10.1002/hed.25781.
Silver Karcioglu AL, et al. Emerging imaging technologies for parathyroid gland identification and vascular assessment in thyroid surgery: A review from the American Head and Neck Society Endocrine Surgery Section. JAMA Otolaryngol Head Neck Surg. 2023 Mar 1;149(3):253-260. doi: 10.1001/jamaoto.2022.4421.
Swift WM, et al. Change in parathyroid hormone levels from baseline predicts hypocalcemia following total or completion thyroidectomy. Head Neck. 2022 Jul;44(7):1588-1595. doi: 10.1002/hed.27057.



 Figure 1. Intrathyroid left inferior parathyroid adenoma with polar blood flow pattern.
Figure 1. Intrathyroid left inferior parathyroid adenoma with polar blood flow pattern. Figure 2. Axial CT non-contrast (left) and arterial phase contrast (right) demonstrating left thyroid tubercle (+) and right superior parathyroid adenoma (*). The parathyroid adenoma is hypodense relative to the thyroid gland on the non-contrast image and avidly enhances on the arterial phase contrast image while the thyroid tubercle is isodense to the thyroid on the non-contrast image.
Figure 2. Axial CT non-contrast (left) and arterial phase contrast (right) demonstrating left thyroid tubercle (+) and right superior parathyroid adenoma (*). The parathyroid adenoma is hypodense relative to the thyroid gland on the non-contrast image and avidly enhances on the arterial phase contrast image while the thyroid tubercle is isodense to the thyroid on the non-contrast image. Figure 3. Minimally invasive left interior parathyroidectomy. Left Inferior parathyroid adenoma (*) and left thyroid lobe (+).
Figure 3. Minimally invasive left interior parathyroidectomy. Left Inferior parathyroid adenoma (*) and left thyroid lobe (+).