More from December 2013 - Vol. 32 No.12

The past 12 months have been ones of transition for Information Technology (IT). During the first part of 2013 an outside assessment and evaluation of IT infrastructure resources and staffing requirements was conducted. This study was robust and looked at all aspects of how Members are served through AAO-HNS/F technology. This full IT review resulted in new strategy and implementation plan.
Structural Changes Ensure Strength for New Growth and Engagement
Two major changes that were of the highest priority included the outsourcing of the helpdesk to free up skilled staffing resources and the move to a cloud-based Infrastructure-as-a-Service (IaaS) environment in answer to increased content and storage needs. These two moves enable the remaining technology staff to move from a platform of technology maintenance to that of engaging technology to forward member needs and resources.
IT’s new focus on providing information and knowledge management is a much broader charge that sustains and supports AAO-HNS/F activities and collaborates with staff. This tectonic shift resulted in the renaming of the business unit to Information and Knowledge Management (IKM) and a new senior director last June.
Improving the Member Experience
With the change in the direction for IKM, focus could now be directed to improving the Academy’s online presence. This included two important projects with Member Engagement and Communications, respectively, to provide the vital integration of technology to member ROI.
★ The Member Portal: ENTConnect
Based on a “best-of-breed” association-centric web platform, the new Member Engagement Portal, ENTConnect, will serve as a resource bank for chairs and committee members, and will enable Members to work more collaboratively, opening up full participation in online communities. Access to the Member Engagement Portal will be based on existing member login credentials. Since access will be restricted to members, this portal will be a place for dialog and discussion, content development and review, assessment and synthesis. ENTConnect is scheduled to go live in the spring of 2014.
★ A New and Responsive Website
It was apparent from the technology assessment that the current website was not what we needed for the future. A new website that will better serve is being constructed and is on track for a roll-out in May 2014. Meanwhile, some improvements to the current site were undertaken. The results are substantive, and the analytics, since these revisions were introduced, reflect an increase in access and usability.
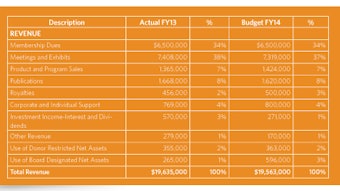
Before selecting a partner to assist in the website redesign, there was an exhaustive review of Request for Proposal responses and in-depth candidate capability presentations. The website redesign project kicked off in Vancouver with member interviews. Communications work in both areas adds an intuitive member experience through a visual taxonomy and branding. Two of the main focus areas for the redesign project are: 1) make our content easier to find and use, both on the site and from search engine results; and 2) have content automatically adjust to the screen size of whatever device is used to access our site. Whether you come to the site from a smartphone, tablet, or full size screen, content on the new website will automatically adjust. The fiscal year July 1, 2012, through June 30, 2013, (FY13) closed with a positive (unaudited) $1.8 million variance from the break-even budget. Overall, revenues were within 1 percent of budget and operating expenses were approximately 10 percent under budget.
With respect to non-operating activities, the return on the managed investment portfolio was nearly 8 percent for the fiscal year. Additionally, a gain of $1.7 million was recorded to adjust for the change in market value of the interest rate swap agreement related to the financing of the headquarters building.
In combination, operating and non-operating FY13 activity increased reserves by $4.1 million. As of June 30, 2013, unrestricted and undesignated reserves were $12.5 million or roughly 65 percent of the operating budget, a level considered within best practices.
The Hal Foster, MD, Endowment, started only three short years ago, now has net assets, pledged, received or to be received in the form of life insurance proceeds or bequests, of $10.3 million as of June 30, 2013. These funds are permanently restricted as endowment principal, the earnings on which are used as directed by the donor at the time the endowment gift was made. Endowment earnings funded almost $60,000 of AAO-HNS/F FY13 programming.
For a copy of the independent audit of AAO-HNS/F’s FY13 financial statements email CHanlon@entnet.org.
In May 2013, the Boards of Directors approved a balanced fiscal year 2014 (FY14) budget. The budgeted revenue is approximately the same as FY13, $19.6 million, reflecting realistic expectations about opportunities for revenue growth. Budgeted expenses reflect inflation adjustments for continuing programs and support expenses. Without additional revenue to meet these increases, the Board carefully analyzed how to maximize member benefits with the available resources and made critical decisions about programs to be carried out in FY14. The budgeting process involved a concerted effort from the elected leadership at every critical decision point, and included several sessions with the Boards of Directors, Executive Committee, and the FISC. The positive results of FY13 reflect good fiscal management, but AAO-HNS/F leadership and staff will continue to watch rising costs against flat revenue growth as strategies for the organization are developed going forward.
-Gavin Setzen, MD, Secretary/Treasure Corporate Funding: $826,000
We continue to work with companies and foundations to fund our mission through the Industry Roundtable (IRT) program, sponsorships, and royalties. We believe that the corporate area has been largely underworked and there is much more opportunity for growth. The Development staff is building relationships with companies and foundations to increase participation in our philanthropic activities. The 2013 Annual Meeting & OTO EXPOSM provided an excellent opportunity to engage corporate leaders in AAO-HNSF.
A financial summary for each program is included with the updates below.
Annual Meeting Sponsorships: $237,000The good news story in the corporate world is the increased interest in annual meeting sponsorships and promotional opportunities. For FY13, we exceeded our budget mark by 63 percent ($236,500 vs. $150,000). Annual meeting sponsorship income is already well ahead of budget for FY14. Our plans include continuing to expand sponsorship opportunities for the 2014 Annual Meeting, as well as approaching potential sponsors earlier in their budget cycle for next year.
Industry Roundtable (IRT): $208,000
General funding for mission support continues to be a challenge for the organization. Due to recent changes in regulations, it is becoming increasingly difficult for industry to support general mission requests, annual meeting support, and educational efforts. Grant requests include the following funding areas: humanitarian aid travel grants, resident leadership grants, CORE, annual meeting educational support, and International Visiting Scholars. We continue to look at ways to revitalize the corporate giving program and are seeking to benchmark our program with programs from similar organizations.
Academy Advantage Royalties: $381,000
The Academy Advantage program continues to offer members select services at discounted rates. For FY13, we closed the year $57,000 (18 percent) over anticipated revenues. Our partnership with HealtheCareers is exceptionally strong and we are seeing good growth in the partnership. In an effort to bolster income, we are working to increase the number of Academy Advantage partners. Life Members
Peter J. Abramson, MD,¹ and Cara Abramson
Kenneth W. Altman, MD, PhD, and Courtney Altman
American Association of Otolaryngologists of Indian Heritage
Vijay K. Anand, MD
J. Noble Anderson, Jr., MD
Seilesh Babu, MD, and Abbey Crooks-Babu, MD
Byron J. Bailey, MD, and Margaret Bailey
Robert W. Bastian, MD, and Jan Bastian
Neal S. Beckford, MD
Leslie Bernstein, MD, DDS
Nikhil J. Bhatt, MD,1* and Anjali Bhatt, MD
Neil Bhattacharyya, MD, and Anjini Bhattacharyya, MD
Andrew Blitzer, MD, DDS
Mark E. Boston, MD
Marcella R. Bothwell, MD
I. David Bough, Jr., MD
Linda S. Brodsky, MD
Robert E. Butler, MD
C. Ron Cannon, MD, and family
Sujana S. Chandrasekhar, MD,* and Krishnan Ramanathan
Ajay E. Chitkara, MD
Sukgi S. Choi, MD,1 and Charles F. Monk, Jr.
Felix W. K. Chu, MD
Noel L. Cohen, MD, and Baukje Cohen
Robin T. Cotton, MD
James Croushore, MD
James C. Denneny III, MD1
David R. Edelstein, MD, and Ms. Eve Lesser
David E. Eibling, MD
Lee D. Eisenberg, MD*, MPH, and Nancy Eisenberg
Janelle A. Y. Engel, MD, and E. Rodney Engel, MD
Deborah J. Freehling, MD
Lisa T. Galati, MD
Raghuvir B. Gelot, MD, and Carolyn Gelot
Samuel J. Girgis, MD
Michael E. Glasscock III, MD
Jack L. Gluckman, MD, and Vickie Gluckman
Steven M. Gold, MD
Barbara Goldstein, PhD
Rebecca D. Golgert, MD
Mary E. Gorman, MD
Thomas A. Graves, MD
Anna Kristina Elise Hart, MD, and William Todd Harder
Jack V. Hough, MD (decd.)
John W. House, MD*
Stacey L. Ishman, MD,* and Jim McCarthy
Barry Jacobs, MD, and MaryLynn Jacobs
Jonas T. Johnson, MD, and Janis Johnson
Srinivas R. Kaza, MD
David W. Kennedy, MD
Darius Kohan, MD
Frank C. Koranda, MD
Alan David Kornblut, AB, MS, MD, and Alfred Kornblut, CAPT MC USNR-RET (decd.)
Jamie Koufman, MD
Dennis H. Kraus, MD
Helen F. Krause, MD (decd.)
Vandana Kumra, MD
Ronald B. Kuppersmith, MD, MBA, and Nicole Kuppersmith
Rande H. Lazar, MD, FRCS
Thomas B. Logan, MD, and Jo Logan
Rick G. Love, MD
Frank E. Lucente, MD
Rodney P. Lusk, MD, and Constance C. Lusk, RN
Sonya Malekzadeh, MD1
Martha Entenmann Tinnitus Research Center, Inc.
Phillip L. Massengill, MD*
Pravina and Dinesh C. Mehta, MD
Ralph B. Metson, MD
James L. Netterville, MD1
David R. Nielsen, MD,1 and Rebecca C. Nielsen, RN
Michael M. Paparella, MD, and Treva Paparella
Spencer C. Payne, MD*
Angela M. Powell, MD
Eileen M. Raynor, MD
Richard M. Rosenfeld, MD, MPH¹
Steven H. Sacks, MD
Harlene Ginsberg and Jerry M. Schreibstein, MD¹
Michael D. Seidman, MD, and Lynn Seidman
Gavin Setzen, MD,¹ and Karen Setzen
Donna E. Sharpe, MD
Abraham Shulman, MD
Herbert Silverstein, MD
William H. Slattery III, MD
Nancy L. Snyderman, MD
James A. Stankiewicz, MD
J. Pablo Stolovitzky, MD, and Silvia P. Stolovitzky
Krishnamurthi Sundaram, MD
Duane J. Taylor, MD¹
Dana M. Thompson, MD, MS
Elizabeth H. Toh, MD
Betty S. Tsai, MD
Ira David Uretzky, MD,* and Beth J. Uretzky
P. Ashley Wackym, MD, and Jeremy Wackym
Pell Ann Wardrop, MD*
Richard Alan Weinstock, DO, and Cheryl Weinstock
Leslie K. Williamson, MD
Lorraine M. Williams-Smith, MD, MPH, FACS
David L. Witsell, MD, MHS
Peak Woo, MD
Geoffrey L. Wright, MD
Ken Yanagisawa, MD,* and Julia Shi, MD
Jay S. Youngerman, MD* and Toni Youngerman
Mark E. Zafereo, Jr., MD
Patron Members
Phyllis B. Bouvier, MD
Hung J. Kim, MD
William M. Luxford, MD
Eugene N. Myers, MD, FRCS, Edin (Hon.)
Rance W. Raney, MD
Sustaining Members
Reginald F. Baugh, MD
William R. Bond, Jr., MD
Peter C. Bondy, MD
Amelia F. Drake, MD
Marvin P. Fried, MD
Michael Friedman, MD
Clarence W. Gehris, Jr., MD
Carlos Gonzalez Aquino, MD
Joseph E. Hart, MD, MS
Stephanie Joe, MD
Alan J. Johnson, MD
Romaine F. Johnson, MD
Nedra H. Joyner, MD
C. Ramadas Kamath, MD
Timothy D. Knudsen, MD
Lisa A. Liberatore, MD
James A. Manning, MD
Edith A. McFadden, MD, MA,
Bert W. O’Malley, Jr., MD
Robert B. Parke, Jr., MD, MBA
Karen T. Pitman, MD¹
Lisa Perry-Gilkes, MD¹
Anna M. Pou, MD*
Ravi N. Samy, MD
Adam M. Shapiro, MD
Carl H. Snyderman, MD, MBA
Sanford C. Snyderman, MD
Joseph R. Spiegel, MD
Jamie Stern, MD
Michael G. Stewart, MD, MPH¹
Mariel Stroschein, MD
Debara L. Tucci, MD
Sunil Ummat, MD, FRCSC
Winston C. Vaughan, MD
Randal S. Weber, MD
Richard Alan Weinstock, DO
Daniel L. Wohl, MD
Stephen Kenneth Wolfe, MD
Rhoda Wynn, MD
Lauren S. Zaretsky, MD¹
Members
Gregory M. Abbas, MD
Daniel P. Akin, MD, PhD
Patricia Allen
Joel N. Anthis, MD
Nancy H. Appelblatt, MD
Richard G. Areen, MD
Oneida A. Arosarena, MD
James E. Arnold, Sr., MD
Moises A. Arriaga, MD
Jonathan E. Aviv, MD
Douglas D. Backous, MD
Sean B. Bailey, MD
Dole P. Baker, Jr., MD
James G. Barlow, MHA
David M. Barrs, MD
David D. Beal, MD
Michael S. Benninger, MD
Peter D. Berman, MD
Philip Bernstein, MD
Todd Blum, MHA, MBA, CMPE
James H. Boyd, MD
Derald E. Brackmann, MD
Jean Brereton, MBA
R. Bruce Buechler, MD
Lawrence P. A. Burgess, MD
Mark E. Carney, MD
Eric S. Carter, MD
Roy R. Casiano, MD
Osmund T. Chan, MD
C. Y. Joseph Chang, MD
A. Craig Chapman, MD
Khalid Chowdhury, MD, MBA
Randall A. Clary, MD
Donald J. Clutter, MD
Stephanie Cordes, MD
Susan R. Cordes, MD
Anthony J. Cornetta, MD
Stephen P. Cragle, MD
Donald E. Crawley, MD
Roberto A. Cueva, MD
Lawrence J. Danna, MD
Kent G. Davis, MD
John M. DelGaudio, MD
Jennifer Derebery, MD
Craig S. Derkay, MD
Daniel G. Deschler, MD
David Devorkin, MD
Elizabeth A. Dinces, MD
Linda J. Dindzans, MD
H. Peter Doble, II, MD
Jeff Dudley
Jolene Eicher
Wayne B. Eisman, MD
John R. Emmett, MD
Moshe Ephrat, MD
Stephanie J. Epperson, PA-C
David A. Evans, MD
Jose N. Fayad, MD
Ilana Feinerman, MD
Berrylin J. Ferguson, MD
Valerie A. Flanary, MD
James W. Forsen, MD
Keith D. Forwith, MD
Ramon A. Franco, Jr., MD
Robert K. Gaughan, MD
James Geraghty, MD
Marion B. Gillespie, MD
Douglas A. Girod, MD
Robert A. Glazer, MPA
Cameron D. Godfrey, MD
David A. Godin, MD
Mohammed A. Gomaa, MD
Barbara Salmon Grandison, MBBS
Iain L. Grant, MB ChB
James C. Grant, MD
Daniel Grinberg, MD
Eli R. Groppo, MD
John R. Gross, FHFMA
John J. Grosso, MD
Benjamin Gruber, MD, PhD
Trevor G. Hackman, MD
Steven D. Handler, MD, MBE
Scott H. Hardeman, MD
Brenda Hargett, CPA, CAE
Willard C. Harrill, MD
James M. Hartman, MD
Ronald H. Hirokawa, MD
Barry Hirsch, MD
Kenneth M. Hodge, MD
Richard S. Hodgson, MD
G. Richard Holt, MD, MSE, MPH
John R. Houck, Jr., MD
Paul M. Imber, DO
Lisa E. Ishii, MD, MHS¹
Tracy F. Jakob, MD
Gina D. Jefferson, MD
Garfield Johnson III, MD
Daniel L. Jorgensen, MD
V. Vasu Kakarlapudi, MD
Michael J. Kearns, MD
David J. Kiener, MD
Haena Kim, MD
James F. Kimbrough, MD
Matthew T. Kirby, MD
James J. Klemens, MD
Mimi S. Kokoska, MD
Howard S. Kotler, MD
Greg Krempl, MD
John H. Krouse, MD, PhD¹
Alice L. Kuntz, MD
Denis C. Lafreniere, MD¹
Christopher D. Lansford, MD
Pierre Lavertu, MD
Amy D. Lazar, MD
Patty Lee, MD
Marc J. Levine, MD
Steven B. Levine, MD
Craig M. Litman, MD
Richard S. Litman, MD
James H. Liu, MD
Philip G. Liu, MD
Long Island Society of Otolaryngology
Howard W. Lowery, MD
James D. Lowery, MD
Keith Lynn
Allen Mackley
Robert H. Maisel, MD
Laurie E. Markowitz Spence, MD
Theodore P. Mason, MD
Becky McGraw-Wall, MD
Benjamin M. McGrew, MD
Jeanne McIntyre, CAE
Kevin X. McKennan, MD
Claude A. McLelland, MD
Brian J. McKinnon, MD, MBA
Gorden T. McMurry, MD
G. Walter McReynolds, MD
Alan G. Micco, MD
Donna J. Millay, MD
Richard T. Miyamoto, MD, MS
Walter P. Moore III, MD
C. Elliott Morgan, MD, DMD
John R. Morris, MD
Samantha Marie Mucha, MD
J. Gail Neely, MD
Donald E. Newland, MD
Mark L. Nichols, MD
Brian Nussenbaum, MD
Rick Odland, MD, PhD
Randall A. Ow, MD
John F. Pallanch, MD
Bradford S. Patt, MD
James K. Pitcock, MD
Christopher P. Poje, MD
Shannon P. Pryor, MD
Robert Puchalski, MD
Frederic A. Pugliano, MD
Gregory W. Randolph, MD
John S. Rhee, MD. MPH1
Brent E. Richardson, MD
Eben L. Rosenthal, MD1
Michael A. Rothschild, MD
Ron Sallerson
Thomas A. Salzer, MD
Robert T. Sataloff, MD, DMA
James E. Saunders, MD¹
B. Todd Schaeffer, MD
Cecelia E. Schmalbach, MD
Seth R. Schwartz, MD, MPH
Merry E. Sebelik, MD
Michael Setzen, MD
Ryan K. Sewell, MD
Rahul K. Shah, MD
Lee M. Shangold, MD
John J. Shea, Jr., MD
Paul F. Shea, MD
Clough Shelton, MD
William H. Sher, MD
Michael R. Shohet
Stanford M. Shoss, MD
Steven D. Shotts, MD
Richard V. Smith, MD
Gary M. Snyder, MD
Robert J. Stachler, MD
J. Gregory Staffel, MD
Wendy B. Stern, MD
John P. Sugrue, MD
Gerald D. Suh, MD
Fred F. Telischi, MD
David J. Terris, MD
Charles B. Tesar, MD
Evan J. Tobin, MD
James S. Toung, MD
Christopher L. Vickery, MD
Michael C. Vidas, MD
Eugenia M. Vining, MD
Richard W. Waguespack, MD¹
Marilene B. Wang, MD
Manish K. Wani, MD
Mark K. Wax, MD*
Julie L. Wei, MD
Samuel B. Welch, MD, PhD
W. Andrew Wells, MD
Donald V. Welsh, MD
Steve West, MD
Stephen J. Wetmore, MD
Gayle E. Woodson, MD
Douglas L. Worden, MD¹
Eiji Yanagisawa, MD
Stanley Yankelowitz, MD
Kathleen Yaremchuk, MD¹
John K. Yoo, MD
Bevan Yueh, MD, MPH
Lauren S. Zaretsky, MD¹
Karen B. Zur, MD
Young Physician Members
Meredith E. Adams, MD
Nadir Ahmad, MD
Kyle P. Allen, MD, MPH
Christina Baldassari, MD
Margo M. Benoit, MD
Nathan A. Deckard, MD
Jayme R. Dowdall, MD
Charles S. Ebert, Jr., MD, MPH
Tamer Abdel-Halim Ghanem, MD, PhD
Ayesha N. Khalid, MD
Oleg V. Kravtchenko, MD
Alf Bjarne R. Lilleaas, MD
Jeffrey C. Liu, MD
Amber U. Luong, MD, PhD
Kelly Michele Malloy, MD
Nikhila P. Raol, MD
Sarah L. Rohde, MD
Marisa A. Ryan, MD
Jennifer Setlur, MD
Ryan K. Sewell, MD
Lawrence M. Simon, MD
Michael C. Singer, MD
Lee P. Smith, MD
Maria V. Suurna, MD
Monica Tadros, MD
Jonathan Y. Ting, MD
Julie L. Wei, MD
Eric P. Wilkinson, MD
Erika A. Woodson, MD
Jay A. Yates, MD
Estelle S. Yoo, MD
Nina S. Yoshpe, MD
Philip B. Zald, MD
Staff Members
Anonymous
Paul Bascomb
Jean Brereton, MBA
David Buckner
Lani Cadow
Mary Pat Cornett, CAE, CMP
Nancy D’Agostino
Brenda Hargett, CPA, CAE
Jenna Kappel, MPH, MA
Thomas Killam, CAE
Estella Laguna
Kathy Lewis
Catherine R. Lincoln, CAE, MA (Oxon)
Heather McGhee
Jeanne McIntyre, CAE
Mary McMahon, CFRE
David R. Nielsen, MD¹
Ross Rollins
Ron Sallerson
Audrey E. Shively, MSHSE, MCHES, CCMEP
Joy L. Trimmer, JD
Pamela S. Wood, MBA, SPHR
As of October 9, 2013
¹ designates current Board of Director member
* designates Development Committee member Individual Giving Hits New Heights
Under the leadership of Nikhil J. Bhatt, MD, Coordinator for Development, the Development Unit has actively worked to increase individual giving to the Foundation. The members of the Development Committee have engaged in promoting the work of the Academy and Foundation and have been instrumental in opening doors and making introductions to potential new donors. The Unit instituted new activities in order to achieve its goals.
Champagne Reception: A donor stewardship and cultivation event was held during the AAO-HNSF 2013 Annual Meeting & OTO EXPOSM. The purpose of the Champagne Reception was to thank donors giving at the highest levels and to encourage active Academy members to upgrade from general Millennium Society member donations ($1,000) and move into the ranks of those contributing at the highest tier of philanthropic giving. This inaugural event was successful with multiple participants donating to the Millennium Society. Plans are already under way for next year’s Annual Meeting.
Young Physician Leadership Grants: The Development Committee determined that successfully obtaining Hal Foster, MD Endowment or Millennium Society Life Member gifts in the future requires engaging our young physician members now. This demographic is defined as those members eight years out of residency or fellowship training and up to 40 years old. To support this goal, three Young Physician Leadership Grants were provided for this year. Each were given as two $500 travel stipends to be applied equally to help with the expenses of attending the AAO-HNSF 2013 Annual Meeting & OTO EXPOSM and the 2014 Leadership Forum. The three grantees attended various committee meetings at the Annual Meeting and have plans to become more engaged in the Academy/Foundation. The plan is to expand upon this program for FY15.
Gifts from Individuals: $323,000
Millennium Society: The Development staff has been engaged in an effort to secure Millennium Society giving in FY 2013. The focus continues to fully engage the Board, as well as the Development Committee, in soliciting Millennium Society support. Development Committee members have contacted donors who have lapsed in their giving and encouraged their renewed support. As we close the books on the AAO-HNSF 2013 Annual Meeting & OTO EXPOSM, we have 428 confirmed Millennium Society members.
Partners for Progress Participation: The Partners for Progress program continues to be an important source of our annual fundraising success. See the current Partners for Progress partners listing. As a forum for the exchange of information, Partners for Progress members have participated in conference calls with members of the AAO-HNSF staff leadership on a bi-monthly basis. At the Partners for Progress Annual Roundtable, members are provided the opportunity to network in person.
HAL FOSTER ENDOWMENT GROSS
Hal Foster, MD Endowment: Hal Foster donations are still being actively pursued. We are working to increase the number of prospects in the pipeline and close on some of the potential donors who have expressed an interest in the last few years, but have not yet made a commitment. On September 1, Steve Church of Creative Financial Concepts, Inc., became our referring agent for planned giving.
Total Hal Foster, MD Endowment $10,340,000
Hal Foster, MD Endowment
Significant Gifts Received This Year
Planned Gifts-Life Policies
$287,000
Planned Gifts-Bequests
$614,000
Paparella Distinguished Award Endowment
$160,000
Byron J. Bailey, MD and Margaret Bailey
Humanitarian Travel Grant Endowment
$50,000
Harry McCurdy, MD Resident Leadership Endowment
$25,000
Women in Otolaryngology Endowment
$14,600
Diversity Endowment
$6,775
Harry Barnes Society Endowment
$6,050
Total Endowment Gifts FY13
$1,163,425 International Engagement
Coordinator for International Affairs, Gregory W. Randolph, MD, reports that roughly 10 percent (and growing) of the Academy’s membership is from outside of the United States, with the largest representation from Canada, Brazil, Japan, Germany, Mexico, Portugal, and the United Kingdom. Engagement opportunities for our International members include writing opportunities for the Bulletin and Journal, as well as attending regional caucuses around the world. This past year saw enhanced communications between the Academy and its 54 International Corresponding Societies Network. The Academy welcomed its four guest countries to the Annual Meeting—Canada, Kenya, Nigeria, and Thailand. And for the first time, the Academy featured a popular Latin America Webcast at the Annual Meeting that attracted hundreds of participants from more than 16 countries, and convened its first International Assembly, which was well attended. Through the International Visiting Scholars (IVS), the Academy offers a limited number of scholarships to junior academics from developing countries. In addition, there are scholarships from Indian ENTs (Indian IVS), a Latin American ENT (de la Cruz IVS) a woman ENT (Nancy L. Snyderman, MD, IVS), and others specifically designated. This year, 12 International Visiting Scholarships were awarded.
Get Involved: Get the Recognition You Deserve!
The Academy’s Honor Awards program is our way of recognizing meritorious service to members. These are earned through your engagement in Academy activities. Through this program, this year 54 members were recognized with an Honor Award, and 20 members were presented with the Distinguished Service Award. Many other awards and recognition are prevalent as you engage with the Academy.
Our committees strive for excellence. This year, three committees were recognized for being “model committees” for their outstanding performance, leadership, and commitment to the goals and mission. Those committees were Allergy, Asthma, and Immunology Committee; Geriatric Otolaryngology Committee; and the Women in Otolaryngology Research and Survey Committee. With more than 70 special interest and Academy standing committees, there are hundreds of opportunities to become involved as has Board member and Ethics Committee Chair, Lauren Zaretsky, MD, for example.
On November 1, the call for committees was made available to members. This allows all members an equal opportunity to indicate their desire to become involved in the future of the Academy for the 2014 committee year. New resources are being launched to make involvement easier and more effective. Development is under way for a new member engagement web portal to make involvement in committees and Academy activities much more convenient for everyone involved.
Humanitarian Efforts
Engaging in the Academy is not only done at home. Huge contributions can also be made abroad through surgical missions, visits to teach newer surgical technologies (e.g., endoscopic sinus surgery), or research efforts to understand the scope of ENT diseases in developing countries. Awards and recognition is well deserved through our members’ commitment to Humanitarian efforts. This year, the Academy’s Distinguished Award for Humanitarian Service was awarded to James E. Saunders, MD, in recognition of his exemplary life-long dedication to the otologic and hearing healthcare for patients worldwide, particularly those in Nicaragua, and for the education and training of a generation of otolaryngology staff and residents in ear surgery. In addition, 29 Humanitarian Travel Grants were awarded to residents and fellows-in-training in 2013 to offer services in 15 less-developed countries. In addition to the grants, this year the awardees had the opportunity to provide educational tools and other “members-only” materials from the Academy to train their colleagues in these countries.
Women in Otolaryngology (WIO) Section
Created in 2010, the WIO Section offers women otolaryngologists the opportunity to strengthen their career support systems and skills through networking events, professional development, and mentoring programs. As with the SRF Section, all women who are members of the Academy are automatically members of the WIO Section. Through its leadership infrastructure, there are ample opportunities for members to demonstrate their leadership abilities and influence the Academy’s future. This year, the Section initiated and increased networking for Women in Otolaryngology via electronic and written communications, programs and speakers. Christina Surawicz, MD, was well received as the guest speaker at the WIO General Assembly in Vancouver, addressing issues of importance to women in leadership positions. More than 250 members attended the event—a record crowd.
Specialty Society Advisory Council (SSAC)
SSAC is vital to the Academy as it serves as a conduit for improved communication and identification of shared opportunities for the Academy and the otolaryngology specialty societies. This past year, SSAC, led by Albert L. Merati, MD, made some changes to its Governing Articles, now providing for a two-year term for its chair, which will enhance the effectiveness of the council and provide consistency in strategy.