More from July 2014 - Vol. 33 No. 07
“Guidelines empower clinicians to advocate for the best clinical care on behalf of their patients, and are often the perfect antidote to denials by insurers of care that is evidence-based yet deemed ‘medically unnecessary’ based on proprietary criteria.”
Richard M. Rosenfeld, MD, MPH
AAO-HNSF Senior Consultant for Quality and Guidelines
April 2014, Richard M. Rosenfeld, MD, MPH, was told that Cigna denied a request for inpatient stay as “medically unnecessary” for a 3-year-old child who was scheduled for tonsillectomy. The child had a sleep study that showed severe obstructive sleep apnea, using criteria defined in the AAO-HNSF Polysomnography clinical practice guideline (CPG). As per the guideline, this type of child should have inpatient observation because they are at high risk of desaturation and may need respiratory support.
When Dr. Rosenfeld had a peer-to-peer discussion with the Cigna physician, he began by stating that according to criteria used by Cigna this did not require inpatient admission. He then referred the Cigna physician to the AAO-HNS website, helped him navigate to the Polysomnography CPG, and find the specific key action statement (KAS) that discussed inpatient admission.
The Cigna doctor was quite impressed with the CPG, admitted that he was unaware of its existence, and stated he would update the criteria used by Cigna to be consistent with the CPG recommendation for inpatient care. He then approved the child for an inpatient stay. 
Jason A. Showmaker, MD
Last October I traveled with World Medical Mission to Kenya to perform cleft lip and palate repairs at AIC-CURE International Children’s Hospital in Kijabe, Kenya. Situated on a mountainside rimming the Great Rift Valley and 31 kilometers west of Nairobi, this geographically isolated hospital is a busy hub of craniofacial cleft repair. Teams travel there three times each year to allow for patient follow up and to provide much needed repairs for poor families and their affected children. Dr. Chang has been travelling there annually since 2005 and this year I was allowed to join him and two other otolaryngologists, Jeffrey Neal, MD, and Cameron Kirchner, MD, to learn the challenging but rewarding art of repairing clefts. I have been interested in humanitarian medicine for many years but this was my first opportunity to travel as a physician and provide much needed care.
We operated out of CUREHospital which was staffed mostly by Kenyan nationals and a handful of missionary physicians from around the world. The hospital and operating rooms ran efficiently and required very little “pushing” on our end. The hospital had been broadcasting daily radio announcements of our arrival and the day we arrived our clinic was packed with parents and their children. Within an hour of arriving, we were already operating on patients who had arrived the night before, gotten lab work, and had been NPO in anticipation. We ran two operating rooms five days a week that out of necessity functioned with very little waste. The anesthesia machines were old but functioning and the cleft trays were well-used but complete. There was routine re-sterilization of non-reusable products such as electrocautery tips which had long since lost their Teflon coating. Endotracheal tubes and suction tubing were stained yellow from multiple sterilizations with betadine and frequently the suction tubing would collapse because the tubing walls were weakened by frequent use. If a suture was opened but not used it was placed in a sterile container in the corner of the room for use in a subsequent case. Surgical sponges were made of washable material which was sterilized along with the drapes. We brought our own IV antibiotics, oral amoxicillin and donated suture. Any suture approaching its expiration date was donated to the hospital.
The hospital staff was glad to have us there and really made the experience enjoyable for us.
There were two anesthesiologists, well-trained scrub techs, and compassionate nurses who were all Kenyans with years of experience working together at the hospital. In the wards, a single large room with 20-plus beds, daily praise and worship led by the hospital staff filled the halls with beautiful music as we drank tea between cases.
As welcoming as the hospital staff was, I was struck by how little emotion the parents showed after their children had their operations. At times it seemed to border on apathy and it really made me and the rest of our team wonder why they weren’t more excited. I came on this trip to serve and learn. I really wasn’t seeking their gratitude but when there was such little outward evidence of their appreciation I have to say I was surprised. In speaking with the hospital staff we learned that in Kenya a sign of true strength is to be unwavering in one’s emotion. To scream, shout, clap, and dance is entirely out of character and actually laughable to them. Instead the mothers accepted their children back into their arms with solemn gratitude, their most honorable display of strength.
The Kenyans showed their strength, and all the while I was getting mine back. The hours were long but my energy and desire to serve increased throughout the trip. Five months later I still reflect on this trip and find renewal. I am a better resident and better physician today because of this trip. I want to sincerely thank the AAO-HNSF Humanitarian Efforts Committee for its grant that made this trip possible. These two weeks were a gift given to me that I will never forget. Susan R. Cordes, MD
Bruce H. Campbell, MD
Debara L. Tucci, MD, MBA
As part of the greater AMPATH Kenya Program, our nine-member team traveled to Eldoret in western Kenya, in February 2014 to deliver medical and surgical care and build on existing relationships in the program. AMPATH (Academic Model for Providing Access to Healthcare) was initiated by Indiana University (IU) physicians in 1989 as a partnership between IU and Moi University School of Medicine. MoiUniversity and its hospital, Moi Teaching and Referral Hospital (MTRH) in Eldoret, provides the only academic medical center for over three million people. The partnership between IU and MoiUniversity has flourished and expanded to include multiple specialties including otolaryngology.
One of the main tenets of AMPATH is to provide education and research but to always “Lead with Care.” With that concept in mind, otolaryngologist/head and neck surgeons have traveled to Kenya once or twice each year since 2009 to provide much-needed surgical care and education. Currently, otolaryngology has the longest waiting time for elective surgery at MTRH, and our team was able to perform 35 procedures and, in the process, teach surgical technique and enhance the already very solid partnership between the American and Kenyan otolaryngologists.
The American team consisted of Susan Cordes, MD (Indiana University), Bruce Campbell, MD (Medical College of Wisconsin), Debara Tucci, MD (Duke University), and Jack Coleman, MD (former chair of plastic surgery at IU), as well as nurses and IU medical student (and otolaryngologist-to-be), Joel Franco. We had the privilege of working with MTRH otolaryngology colleagues Titus Sisenda, MMed, Henry Nono, MMed (AAO International Visiting Scholar 2012), and
Denge Makaya, MMed, and performed a wide range of surgeries, including thyroidectomies, nasal/sinus surgeries, cleft lip repairs, excision of cystic hygromas, facial/neck flap reconstruction, Sistrunk procedures, and a total laryngectomy. In addition, Debara Tucci met with key individuals to explore initiation of a hearing healthcare program for the region.
Based on our past experience with these trips, we brought most of the necessary supplies, but still ran out of some of the seemingly most basic of items (e.g., suction tubing connectors, Mastisol, steri strips, etc.). Though we wish we could have stayed until the last of the patients had been released from the hospital, we confidently left the care of the patients in the hands of our Kenyan colleagues and continue to receive regular updates on their progress.
Looking to the future, we plan to continue these trips and perhaps increase the frequency. Our Kenyan colleagues are
exploring whether they might develop an otolaryngology residency program, which would be the second in Kenya. Our first joint research project has been submitted for review at both institutions, and we will continue to raise funds to further the educational experiences for our Kenyan otolaryngology colleagues.
Traveling to a distant land to perform surgery in a difficult environment is a challenge; however, the rewards of providing care that otherwise might not be possible far outweighs any hardship on our part. Experiences such as this trip really help crystallize what is important and valuable. It is so easy to get caught up in the pressures and frustrations of everyday life in the U.S.; however, in the greater world, there is more hardship than most of us can imagine, and the ability to affect the lives of these patients and our Kenyan colleagues is truly a gift. We are proud that so many otolaryngologists participate in these noble ventures and that the AAO is so supportive of humanitarian efforts. Anyone who has ever participated in one of these trips knows exactly what we mean, and for anyone who has not, we hope you take the opportunity. The American Academy of Otolaryngology—Head and Neck Surgery Continuing Professional Development (CPD) Program has been analyzing the education needs, demographics, and career stages of its target audience. The goal of this analysis has been to construct a user experience that is focused on the demands of the individual specialties, yet comprehensive enough to provide a broad curriculum for the entire medical specialty. In order to actively engage this learner audience, however, AAO-HNSF must first have the correct tools to enable the design of activity formats that are built to align with diverse learner preferences. Plans are in process to build a new a Learning Management System (LMS) which will provide such tools and act as a hub through which the Foundation will create and deliver learning opportunities. The LMS will allow members and others in the greater healthcare community to design a customized education portfolio that meets their individual needs.
The objectives of our LMS implementation and operation are to:
Consolidate the Academy’s education resources and services under one easily accessible site, maintained and serviced by a single vendor.
Expand the Academy’s education library to include innovative new formats that engage the learner in a more interactive, individualized education experience.
Grow the Academy’s course participation by engaging new target audiences and encouraging repeat use.
A new LMS will offer many features that will enrich members’ learning experience. These include the ability to:
Recommend courses to users based on their professional interests and background.
Support certified education, specifically AMA PRA Category 1 Credit™.
Support the development of communities of practice and enable AAO-HNSF to build online learning communities.
Provide access to a library of high-quality education content on a variety of topics.
Build courses with content authoring tools: images, videos, and other file-based content can be embedded directly in activities.
Be viewed on any device and support the most recent releases of Chrome, IE, Safari, and Firefox.
Integrate a search function that pulls keywords from all resources on the AAO-HNS/F website.
In addition, a new LMS will support these key strategic education resources.
On Demand Learning and Interactive Platforms—The Foundation will be able to design future education activities that are self-paced, engaging, interactive, and customizable to individual learners. Such activities include patient case scenarios, simulation/gamification, and point-of-care learning.
Assessment Courses/Question Bank—The Foundation will be able to leverage its existing self-assessment resources and established question-writing processes to produce a question bank and other self-assessment modules. The primary target market for these products will be recertifying physicians and residents. Such items as a question-of-the-day, practice tests, and exam prep will be available.
Assessment and Continuing Education for Print Products—The Foundation will be able to maintain a host of print products, many of which will also have a duplicate online “eBook” edition. In order to grant continuing education credit for the print products, the new LMS will be able to support the post-test requirement to grant credit. The LMS would use a unique course identification code printed in each book to allow those who purchase the print product to access the post-test and credit request online.
There are numerous additional administrative benefits to a new LMS that will make our education activity planning and evaluation more robust and meaningful. These benefits include:
Needs Assessment data can be generated through advanced reporting features that correlate pre-test/post-test assessment scores with current literature on practice gaps.
Testing functionalities allow pre-test/post-test scoring along with automated CME/CE credit request and certificate distribution.
Evaluation options for new approaches to collecting needs assessment and user satisfaction data including automatic evaluation distribution and polling/survey widgets.
CME/CE Transcript Generation/Repository gives members the ability to access CME/CE certificates immediately upon completing a course and access to certificates from past activities.
As you know, AAO-HNSF has recently conducted a multiyear member education needs assessment along with a committee-led review of all current activities. As a result of this analysis, along with the introduction of a powerful new LMS, the Foundation stands poised to launch a dynamic, personalized, and flexible professional development platform that will engage our membership as never before. Definition of a Position Statement:
A Position Statement is used to designate a statement, policy, or declaration of the AmericanAcademy of Otolaryngology—Head and Neck Surgery, and Foundation (AAO-HNS/F) on a particular topic or topics. Statements are created to formalize the AAO-HNS/F position on a clinical procedure or medical service with third party payers, for use in state and federal regulatory or advocacy efforts, or to clarify the AAO-HNS/F approval or disapproval of certain practices in medicine. For information about the differences between Position Statements and other quality knowledge products, such as Clinical Practice Guidelines, view the AAO-HNS/F Guidance Documents fact sheet on the website (http://www.entnet.org/default/files/Guidance-Documents.pdf).
How are AAO-HNS/F Position Statements Created and Approved?
Have you ever wondered how a Position Statement is created and what is involved in the process of review and final approval by the Board of Directors? In response to questions like this one the Health Policy department and the Physician Payment Policy (3P) workgroup that oversees the review and maintenance of the Position Statements, published a guidance document for AAO-HNS/F committees with a step-by-step process on how to develop a Position Statement. Notably, this document defines a Position Statement, clarifies its process of development, and clarifies its purpose as an AAO-HNS/F resource. This guidance document can be found on the Academy’s website (http://www.entnet.org/sites/default/files/Position-Statement-Template.pdf). This article provides examples of how members use the resource as an advocacy tool or to clarify the AAO-HNS/F approval or disapproval of certain practices in medicine.
How Are AAO-HNS/F Position Statements Used by Members as a Resource?
Real Examples of how AAO-HNS/F Position Statements are used as a resource include:
Position Statements can be used to advocate with payers regarding coverage policies and issues that members are experiencing with third party payers.
Example: An otolaryngologist has difficulty getting approval for a surgery including uvulapalatopharyngoplasty (UPPP) and midline glossectomy as treatment of obstructive sleep apnea (OSA) in patients where continued positive airway pressure (CPAP) has failed as treatment. As rationale for the denial, the insurance reviewer states that there is a lack of literature supporting this approach. The physician appeals the denial using Academy position statements on UPPP, mid-line glossectomy, and surgical management of OSA. The insurer subsequently reviews the supporting documentation reinforced by peer-reviewed literature to determine whether or not to reverse the denial and approve payment of the claim.
Position Statements are also used to promote the Academy’s position on specific medical procedures.
Example: The Academy published a position statement noting that sinus ostial dilation is an appropriate therapeutic option for selected patients with sinusitis. The statement also includes a list of supporting literature to indicate why we support this procedure as an appropriate option for clinical management. The Academy has provided this Position Statement to dozens of private healthcare insurers and several have reversed their decision of experimental and investigational, and instead, allowed for coverage.
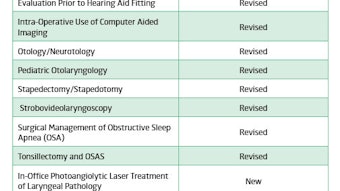
What are the latest New or Revised Position Statements Approved by the AAO-HNS/F Board of Directors?
After an extensive review by AAO-HNS/F committees, the Executive Committee, and Board of Directors, the AAO-HNS/F revised nine, and published three new, Position Statements. The AAO-HNS/F reviews all position statements on a rolling four-year basis. For a listing of the updated Position Statements [Communications insert standard language to drive members to Bulletin online.] The latest updates can be found on the AAO-HNS/F website at http://www.entnet.org/positionstatements.
Any questions about position statements? Email the health policy team at healthpolicy@entnet.org. During the past few years, the Health Policy team has actively worked not only to educate members on the Centers for Medicare & Medicaid’s (CMS) Quality Initiative programs, but also to advocate on behalf of you so your needs and experiences are represented within the programs. This is particularly true with the Electronic Health Records (EHR) Meaningful Use (MU) Incentive Program, and 2014 is no exception. This year is important for a variety of reasons, one being it is the year that CMS plans to publish the notice of proposed rulemaking (NPRM) regarding Stage 3 of EHR MU.
For those members not fully up-to-speed on the EHR MU program, this article includes a brief overview of the program and highlights Academy advocacy efforts as CMS develops Stage 3. [Communications insert standard language to drive members to Bulletin online.] By continuing advocacy efforts, the Health Policy team hopes to help members sort through any confusion associated with the EHR MU program, prepare for increased requirements, avoid penalties, and successfully participate, so you can focus on what matters most: providing excellent patient care.
Did You Know?
Rulemaking is a process that federal government agencies, such as CMS, use when developing governmental regulations. This process requires the opportunity for public comment before final regulations may be made. The Academy submits comments to CMS, and other agencies, on priority issues that impact otolaryngology-head and neck surgeons nationally.
Background
As you may know, the EHR MU was designed by CMS to facilitate the use of EHRs in clinical settings, with the program goals being to promote greater efficiency in healthcare, decrease costs, and improve the communication of medical information as it is shared between providers, regulators, and public health agencies. To meet those goals, eligible professionals (EPs) are expected to demonstrate they are “meaningfully using” their EHRs in such a manner that improves overall quality of care and increases patients’ choice as defined by CMS. In other words, it’s not simply a matter of utilizing EHRs, but rather, EPs and other healthcare professionals are expected to meet a number of thresholds for several objectives, with the requirements increasing as the stages of the program (1, 2, and 3) progress. For the most part, all three stages retain the same basic structure: EPs must report the required number of MU objectives + required number of clinical quality measures (CQMs) + any other reporting requirements.1
For the individual requirements, MU objectives are divided into two types: CORE and MENU. EPs are expected to report on all CORE measures but can choose the required number of MENU measures from a list based upon what best suits that individual’s practice. In addition, the MU objectives vary depending upon which stage of the program an EP is currently participating in. The requirements of each stage are designed to advance that particular stage’s chief goal (i.e., data capturing and sharing, advanced clinical processes, and improved outcomes). Stage 2 is currently underway, but Stage 3 is on the horizon with many new changes likely to impact specialists.
Stage 3
AAO-HNS Comments on HITPC Recommendations for New/Heightened MENU and CORE Measures
The Health IT Policy Committee (HITPC) is the federal advisory committee that makes recommendations to the Secretary of Health and Human Services (HHS) regarding the EHR MU Incentive Program. In spring 2014, the HITPC made several recommendations to CMS regarding Stage 3 requirements, which included many new or heightened MENU and CORE measures. Unfortunately, many of the recommendations are either reliant upon EHR systems that are fully interoperable or are requirements that are poorly suited for specialists, like ENTs.
Since CMS considers the HITPC recommendations when developing their proposed rule, the Academy, along with other specialty societies, worked with the AMA to provide comments to CMS in hopes of changing many of the recommendations. Below is an example of one of the comments submitted by the AAO-HNS on a new MENU measure proposed by the HITPC.
AAO-HNS General Comments on Stage 3: Increasing Costs for Providers
In addition to commenting on the specific measures, the AAO-HNS also noted that while it supports the continued integration of EHRs into the practices of otolaryngologists-head and neck surgeons, it remains extremely concerned that the new and expanded requirements under Stage 3 will be increasingly difficult for otolaryngologists to meet, especially in light of the increased costs associated with meeting the higher standards and the additional maintenance required without the possibility of receiving incentive payments in coming years. The AAO-HNS further commented that because providers are also responsible for the expenses associated with implementing the core, menu and clinical quality objectives, it is imperative that flexibility be built into the program, which is currently lacking. As many can agree, flexibility helps ensure not only the continued adoption of HIT, but also avoids hindrances to patients’ access to quality care.
AAO-HNS Health Policy Team Provides Resources to Members
As rulemaking continues, the AAO-HNS will continue to stay actively engaged in the process and will keep members apprised of all pertinent information relating to the program. Members are also encouraged to stay engaged. View invaluable tools created by the AAO-HNS Health Policy team (available at: http://www.entnet.org/Practice/ONC.cfm) to help you understand the program and prepare your practice:
AAO-HNS EHR MU webpage
AAO-HNS EHR MU Fact Sheet
Members should also stay tuned in to the eNews, HP Update, Bulletin, website, and other outreach tools for any announcements on important changes, deadlines, or other key factors surrounding the program.
1. Please note: This article is designed to provide a brief overview of the EHR MU Incentive Program and does not describe many pertinent aspects, such as the CQM requirements or other requirements that are essential to successfully participating in the program. Because of such, members are encouraged to review the resources listed on the Academy’s EHR webpage to ensure they fully understand the program and its implications.