Research and Quality: Next Steps
The changing landscape of today’s healthcare environment includes an increased focus on reducing costs and improving the quality of care we provide to our patients, in a nutshell, adding value. Many federal quality programs, including the Physician Quality Reporting System (PQRS), Meaningful Use of Healthcare Technology (MU), and Value Based Modifier Program, assess physician performance through quality measurement. The AAO-HNS/F has historically relied on the AMA Physician Consortium for Performance Improvement® (PCPI®) to develop quality measures for otolaryngology-head and neck surgery. Otitis Media with Effusion (OME) and Acute Otitis Externa (AOE) as well as Adult Sinusitis measures were developed in partnership with the PCPI utilizing our Clinical Practice Guidelines (CPG). Moving forward, the PCPI will continue to provide these services to specialty societies but only on a consulting basis. The AAO-HNS/F Board of Directors recently approved as part of its strategic plan the Foundation’s development of future quality measures and the stewardship of existing measures. Similar to our process for CPG development, AAO-HNSF will form a quality measures task force which will work with volunteer experts and staff to identify best practices for quality measure development and for prioritizing medical conditions for which measure development is necessary. We will look to the specialty society leadership to help identify physician volunteers to serve on development panels. This is an exciting new endeavor for the AAO-HNSF and will ensure more meaningful quality measures for our members.. The first measures development project was completed recently with representatives from the American Board of Otolaryngology (ABOto) and Academy research and quality physician leaders and volunteers. The group came together with AMA facilitation, to develop two measures groups (AOE and Adult Sinusitis) utilizing existing measures. A measures group eases the reporting requirements for PQRS as a physician need only report on 20 individual Medicare patients rather than 80 percent of their Medicare patients, the requirement for reporting individual PQRS measures. Physician leaders and staff met with Dan Green, MD, CMS Medical Director to review these measure groups for the 2015 Medicare Physician Fee Schedule. We received favorable feedback and will find out with the fee schedule interim rule release, if the groups were approved. See updates on www.entnet.org.
 Richard W. Waguespack, MD
Richard W. Waguespack, MDAAO-HNS/F President
The changing landscape of today’s healthcare environment includes an increased focus on reducing costs and improving the quality of care we provide to our patients, in a nutshell, adding value. Many federal quality programs, including the Physician Quality Reporting System (PQRS), Meaningful Use of Healthcare Technology (MU), and Value Based Modifier Program, assess physician performance through quality measurement.
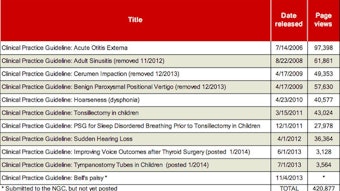
The AAO-HNS/F has historically relied on the AMA Physician Consortium for Performance Improvement® (PCPI®) to develop quality measures for otolaryngology-head and neck surgery. Otitis Media with Effusion (OME) and Acute Otitis Externa (AOE) as well as Adult Sinusitis measures were developed in partnership with the PCPI utilizing our Clinical Practice Guidelines (CPG). Moving forward, the PCPI will continue to provide these services to specialty societies but only on a consulting basis. The AAO-HNS/F Board of Directors recently approved as part of its strategic plan the Foundation’s development of future quality measures and the stewardship of existing measures. Similar to our process for CPG development, AAO-HNSF will form a quality measures task force which will work with volunteer experts and staff to identify best practices for quality measure development and for prioritizing medical conditions for which measure development is necessary. We will look to the specialty society leadership to help identify physician volunteers to serve on development panels. This is an exciting new endeavor for the AAO-HNSF and will ensure more meaningful quality measures for our members..
The first measures development project was completed recently with representatives from the American Board of Otolaryngology (ABOto) and Academy research and quality physician leaders and volunteers. The group came together with AMA facilitation, to develop two measures groups (AOE and Adult Sinusitis) utilizing existing measures. A measures group eases the reporting requirements for PQRS as a physician need only report on 20 individual Medicare patients rather than 80 percent of their Medicare patients, the requirement for reporting individual PQRS measures. Physician leaders and staff met with Dan Green, MD, CMS Medical Director to review these measure groups for the 2015 Medicare Physician Fee Schedule. We received favorable feedback and will find out with the fee schedule interim rule release, if the groups were approved. See updates on www.entnet.org.