More from October 2013 – Vol. 32 No. 10
At its June 22 meeting, the American Board of Facial Plastic and Reconstructive Surgery (ABFPRS) board of directors determined that the following 33 surgeons had met all of the requirements to become ABFPRS diplomates. The action brings the total number of active diplomates to 1,050.
Shervin Aminpour, MD
Dominic M. Castellano, MD
Jen Y. Chow, MD
Kristin K. Egan, MD
Waleed H. Ezzat, MD
Rebecca E. Fraioli, MD
Alexis Furze, MD
Jason M. Guillot, MD
Douglas K. Henstrom, MD
Laura E. Hetzler, MD
Tang Ho, MD
Jared C. Inman, MD
Keith Michael Ladner, MD
Patrick Chase Lay, MD
Jacque Perrin LeBeau, MD
William D. Losquadro, MD
Umang Mehta, MD
Timothy Minton, MD
Jason Moche, MD
Sachin S. Parikh, MD
Shari Reitzen-Bastidas, MD
James M. Ridgway, MD
Alicia R. Sanderson, MD
Maya G. Sardesai, MD
Christopher R. Savage, MD
Ali Sepehr, MD
Anita Sethna, MD
Taha Z. Shipchandler, MD
Christian L. Stallworth, MD
Scott J. Stephan, MD
Samir Undavia, MD
Preston Daniel Ward, MD
Cory Chi-Hong Yeh, MD 
With a record number of firsts, the 4th Conference of the Coalition for Global Hearing Health (CGHH) at VanderbiltUniversity’s BillWilkersonCenter, Nashville, TN, May 3-4, was rated a resounding international success by attendees from 15 countries.
As in past conferences, multiple disciplines around the globe conferred for two days on global hearing healthcare provided in lower-resourced regions.
This year’s “firsts” included:
Offering individual and organizational CGHH membership. Annual individual membership is $25, and organizational memberships are $100 for organizations with offices in HINARI (Health InterNetwork Access to Research Initiative) A and B Category countries, and $250 for organizations in other countries.
Awarding the first travel scholarship to Ned Carter of All Ears Cambodia, who said, “I couldn’t have attended the conference, if it weren’t for this scholarship offered by Bob and Jean Johnson. I am most grateful.”
Awarding 12 portable battery-powered audiometers to humanitarian projects globally, donated by Purdue Pharmaceuticals.
Introduction of a poster session/reception due to an abundance of high quality submissions.
Among many highlights this year, Lady Jean Wilson, OBE, FRCOphth (Hon), gave the conference keynote speech at the historic Travellers Rest Plantation. She founded the Royal Commonwealth Society for the Blind with her husband, Sir John Wilson, and is currently chair of the Hearing Conservation Council; president of the UK Impact Foundation, and vice president of Sightsavers International.
Conference co-organizers, James E. Saunders, MD, Dartmouth Hitchcock Medical, and Jackie L. Clark, PhD, University of Texas at Dallas, have long-established roots in international arenas as humanitarian committee chairs of their professional organizations—the American Academy of Otolaryngology—Head Neck Surgery Foundation and International Society of Audiology, respectively.
Next year’s conference will take place at St. Catherine’s College, Oxford, UK, July 25–26, 2014. To learn more on upcoming or past conferences, visit the CGHH website: http://coalitionforglobalhearinghealth.org or email James.E.Saunders@Hitchcock.org, jclark@utdallas.edu or Conference@CoalitionForGlobalHearingHealth.org. Each year at the Annual Meeting & OTO EXPOSM the eight Foundation Education Committees meet to develop their new work plans. These committees, organized around the otolaryngology specialty areas, take the lead in developing the education activities and knowledge resources produced by the Foundation. In Vancouver, the planning process was organized a little differently than in the past, but equally productive.
As has been discussed earlier, an Education Needs Assessment Initiative was implemented this year. Its purpose is to determine how to best meet the education needs of the Foundation’s members and other constituents. The Initiative began with an Education Committee Survey and SWOT Analysis and also included a review of past education activity participant evaluation data, a business model analysis of all current education activities and knowledge resources, and most importantly, a membership-wide education needs assessment survey, which was conducted in August. Results were summarized and shared with the Education Committees in September.
In order to most efficiently present this important information, a Joint Education Committee Meeting took place on the Saturday before the Annual Meeting. More than 200 committee members met to hear the Education Needs Assessment Summary Report. A joint presentation was given by Education leadership and staff as well as with representatives from LoyaltyResearchCenter, who conducted the membership needs survey for the Foundation.
This joint meeting was a great way to present the information to everyone at the same time and to provide an opportunity for the committees to ask questions. More importantly, it offered everyone the chance to discuss the findings with each other and what the implications are for the future of professional education at the Foundation.
The committees were presented with four outcome objectives from this needs assessment initiative. They were to develop an action plan to improve the member education experience; design education activities that meet the clinical needs of our members; increase member involvement in and satisfaction with education offerings; and enhance member knowledge, competence, and skill in their practice of otolaryngology-head and neck surgery.
Immediately following the joint meeting the individual education committees divided up and met for their traditional annual committee meeting. It was during these individual meetings that the committees discussed how best they could meet these four objectives based on the evaluation and survey data they had just received. This discussion will inform the committees’ 2013-14 work plan.
The results of the year-long analysis will provide useful information to the committees as they plan more focused education activities. The data will help determine not only priority course topics, but the most effective education design and format including the media best used to educate and inform the members. The Education Committees are now tasked with ascertaining how the members need and want to engage in lifelong learning and developing an education and knowledge platform to meet those needs.
Look for the complete Education Needs Assessment Initiative Summary in future issues of the Bulletin and other AAO-HNSF communications. The January Bulletin will be dedicated to the education and knowledge efforts of the Foundation and especially the hard work of the eight Education Committees. Many exciting changes may be underway as we shift our education efforts to best meet the needs of our members.
If you have any suggestions about Professional Education at the Foundation, please email us with your feedback at education@entnet.org.
The outcome objectives from the year-long needs assessment initiative are:
Develop an action plan to improve the member education experience
Design education activities that meet the clinical needs of our members
Increase member involvement in and satisfaction with education offerings
Enhance member knowledge, competence, and skill in their practice Rahul K. Shah, MD, George Washington University School of Medicine, Children’s National Medical Center, Washington, DC
I have often chatted with fellow physicians and Academy members about the massive amount of data that is being accumulated on our practice patterns from not only our own hospitals and payers (private and the government), but from sources such as electronic medical records and even companies that track patient satisfaction scores. As big data becomes more manageable in the digital revolution, the ability to synthesize through hundreds of thousands of records becomes expected and the norm, rather than an anomaly. The major concern is then, what comes of this big data and how is it synthesized and analyzed before it is presented?
A major player in the electronic medical records industry, Practice Fusion®, recently came under fire from practices that used their free platform as there were concerns about the company’s intent to aggregate big data, parcel the data, and sell it for analysis (for example, macro level data on thousands of patients with diabetes could be invaluable for a pharmaceutical company).
There must be similar concern about what is going to happen to the practice of medicine under the extreme scrutiny of the untrained, emotional eye of the observer. For example, what if the big data demonstrates that in my practice region of the greater Washington, DC, area I am an outlier (this is hypothetical of course) for complications? What if the data demonstrated that I had a higher-than-average right-sided post-tonsil bleed rate? Remember, with big data the data can be analyzed and twisted and turned in myriad fashions. So, let us play out the scenario above. What are my patients going to do when they find out that my right-sided post-tonsillectomy bleed rate is higher than my peers in our practice region? Furthermore, what is the hospital going to do about credentialing my focused practice-performance evaluations and my privileges? Will my right-tonsillectomy privileges be rescinded? What if all of my patients who bled in the preceding time period had bleeding diatheses that were neither captured nor reported by those that aggregate our patient data (i.e., lack of risk adjustment)?
This issue is in distinction to doctor’s review sites that are public sites where people blog about their physicians and can give them rankings, such as ZocDoc.com. These sites provide more granular level data that one can argue is actionable. However, the big data being collected about our practice patterns and outcomes is different because it is provided to agencies from hospital administrative staff, and often lacks actionable data or granularity. There can be issues with attribution and coding of cases, which can affect the macro level trend data.
So What Are We To Do?
There are many options, but the two that resonate the most with me is to first, understand the major data reporting repositories so you understand their methodology and how they report out data. Understanding how the data is collected and what it means can help you explain to your patients why the hospital you operate at is below the national benchmarks for specific case types and various other indicators (hospitalcompare.hhs.gov). Once you know where your data and your hospital’s data are being reported, you can speak with the administrative individual at your local hospital that is providing the data to ensure proper and complete case capture.
Finally, we must own our patient’s outcomes and data. There are now data registries where one can sign up through national organizations, such as the AmericanCollege of Surgeons. If we can be stewards of our own data, then we can ensure that it is risk-adjusted, accurate, and reflects our true practice patterns.
On a personal level, this article is even more pertinent, because my real “big brother” is also a pediatric otolaryngologist at Nemours in Wilmington, DE. He can watch his younger brother anytime and pretty soon—with the way that data transparency is coming along, he will not even have to watch me—he can go to the Internet and check my metrics to ensure that I am causing no harm!
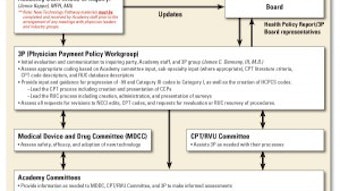
We encourage members to write us with any topic of interest and we will try to research and discuss the issue. Members’ names are published only after they have been contacted directly by Academy staff and have given consent to the use of their names. Please email the Academy at qualityimprovement@entnet.org to engage us in a patient safety and quality discussion that is pertinent to your practice. As members may be aware, the Academy released the New Technology Pathway Application and guidance document in 2010 to provide clarity for members, committees, and industry partners requesting Academy support for revisions to, or the creation of, new Category I and Category III CPT codes. The application can be found at www.entnet.org/Practice/Valuing-CPT-Codes.cfm by clicking on “New or Revised CPT Code Application.” An overview of the process for reviewing these materials is outlined in the figure.
The New Technology Pathway Process was initially developed to provide a more streamlined process, consistent with approaches adopted by other specialty societies. The process requires that the New Technology Pathway Application be completed and submitted to Academy Health Policy staff for any requests for guidance on how to code for a new technology, the development of new CPT codes for services or procedures, or revisions or revaluations of existing codes. The process includes coordination between the Physician Payment Policy Workgroup (3P) and experts from other applicable AAO-HNS committees (e.g., Medical Device and Drug Committee, CPT/RVU Committee, etc.) as a way to incorporate all of the resources and clinical expertise of the Academy in the interest of the members.
Changes to the process were made this year in response to input from submitting stakeholders and were based on experience with the applications received since the inception of the process in 2010. Key changes made this year include:
Implementation of an anti-lobbying policy consistent with the rules and requirements of the AMA CPT Editorial Panel and the AMA RUC.
Requests for information on any AAO-HNS subspecialty committees with which the stakeholder has shared information or has requested support from regarding their application request.
Modified to include requests for support to create a new HCPCS code and modifications to NCCI edits for existing CPT codes.
Modifications to the application to request a clinical vignette for the typical patient undergoing the procedure when a request for a Category I or III code is made.
Requests for any applicable history or background on previous requests for HCPCS or CPT codes associated with the procedure/service outlined in the application.
As the guidance pathway outlines above, all requests are reviewed by 3P, co-chaired by James C. Denneny, III, MD, and Jane T. Dillon, MD, the coordinators for Socioeconomic and Practice Affairs, which is the senior advisory body to Academy leadership and staff on issues related to socioeconomic advocacy, regulatory activity, coding/reimbursement, and practice services/management. 3P evaluates inquiries for new technology coding and requests for new Current Procedural Terminology (CPT) codes, revisions to existing CPT codes, and requests for support of new HCPCS codes. Members of 3P, including Richard W. Waguespack, MD, Bradley F. Marple, MD, and Lawrence M. Simon, MD, represent the Academy on the AMA CPT Editorial Panel’s Advisory Committee. Our CPT representatives advocate for otolaryngology by presenting new and revised CPT codes to the CPT Editorial Panel for inclusion in the CPT code set used for physician billing.
When it comes to valuing CPT codes, 3P serves as the expert consensus panel to analyze surveys completed by Academy members and make recommendations for appropriate physician work and practice expense Relative Value Units (RVUs) to the AMA/Specialty Society Relative Value Update Committee (RUC) for otolaryngology-related codes. The Academy is represented at the RUC by Wayne M. Koch, MD, John T. Lanza, MD, Peter Manes, MD, and Pete Batra, MD. Charles F. Koopmann, MD, MHSA, and Jane T. Dillon, MD, serve as RUC panel members. The RUC makes recommendations on the Relative Value Units (RVUs) of new and revised physician services to the Centers for Medicare & Medicaid Services (CMS). The RUC also performs broad reviews of the Resource Based Relative Value System every five years and rolling reviews of many codes based on screens such as high utilization, frequency of codes used together, and codes not surveyed since the beginning of the RUC process, more than 20 years ago.
We are confident the New Technology Pathway addresses such requests in a manner that is clearly defined, consistent with AMA CPT and RUC guidelines, accounts for the interests and perspectives of all stakeholders, while protecting against undue influence of any group or individual, encourages the collection of reliable data, and promotes efficient, fair reimbursement for our members and appropriate access to new procedures and services for patients. Inquiring parties, including physicians and industry representatives, should send the completed application to Jenna Kappel, the Academy’s director of health policy, at JKappel@entnet.org. The Academy receives daily member inquiries and notifications regarding claim denials and payment policy issues that arise when seeking reimbursement for otolaryngology procedures from private insurers and Medicare. In response, the Academy has a wealth of resources available to members, including: CPT for ENT articles, appeal template letters, clinical indicators, and position statements to help members obtain appropriate reimbursement for various otolaryngology procedures. These resources are available on the Academy’s “Coding Corner,” which is available at http://www.entnet.org/practice/codingResources.cfm.
Due to a large volume of national policy issues submitted to the Health Policy Unit, the Academy works to prioritize and respond to payer coverage issues according to the number of members or geographic regions affected by each policy. Based on time and resources available, the Health Policy department and the Physician Payment Policy (3P) Workgroup may offer assistance for issues affecting many members at the state or national level in cases where the appeals process has been exhausted and resulted in an unsuccessful outcome.
Upon receipt of inquiries regarding private payer denials we work to determine whether the issue is a local or state based, or if it is a national issue that the Academy 3P workgroup should be involved in. Outlined below are the recommended steps for members who encounter difficulty obtaining reimbursement for their services.
Ensure that the service was billed appropriately (e.g., appropriate modifiers used with appropriate CPT codes).
Consult the Academy website for various resources to assist with an appeal for a specific service. Some helpful resources include:
CPT for ENT coding guidance articles: http://bit.ly/CPT4ENT
Code changes for CY 2013: http://bit.ly/2013codes
Information on NCCI /MUE Edits: http://bit.ly/ENTcoding
Audiology FAQs: http://bit.ly/audiologyFAQs
E/M Documentation guidelines: http://bit.ly/EMguide
Template payer appeal letters for services commonly denied: http://bit.ly/entappeals
Do you have the local payer policy for the procedure? Access the carrier’s website, logging in as a provider, and search for the policy relevant to your geographic jurisdiction.
The Academy cannot represent physician members individually on each issue with payers, but health policy staff does track the issues and monitors whether a local or state issue becomes a national issue that 3P should address on behalf of all members.
Talk to the medical director to get more information on the rationale used for the denial. We have found that many times there is a better outcome when the local AAO-HNS physician members who work directly with the payer’s medical director on issue resolution address a local issue.
If 3P determines that the issue is a regional or national issue that could affect many otolaryngologists, information on the payer policy and the rationale used by the payer’s medical director is helpful for Health Policy staff to determine if this is a local issue. If that information is available to forward, that is helpful for 3P to know as well. All of this information helps us as we determine the best course of action for your request, and track members in certain states who are having difficulty with specific payers.
To find out how widespread an issue is, we strongly recommend you work with your state society of otolaryngology-head and neck surgery, Board of Governors representatives, and state medical society to report the issue so they may attempt to assist you. They may also be able to provide a better idea of how widespread an issue is among providers in the area. You can access contact information for several state otolaryngology societies on our website at http://www.entnet.org/Community/BOGSocieties.cfm?View=State (Login required).
We strongly recommend that you also contact others in your community to determine if they are having the same issues. The Academy coordinates with the Association of Otolaryngology Administrators (AOA) Advocacy and recommends that you reach out to the AOA [www.oto-online.org] to determine if other practices are having similar issues. Since state issues are usually best resolved with leaders at the state level, we recommend administrators and their physicians contact the AOA to receive resources that others may have used in other states to resolve the issue. The Academy offers the AOA the resources that we have available, such as a comment letter, if 3P determines it could affect many members and would help with advocacy efforts.
For Medicare payment issues, we often recommend you contact the Medicare Administrative Contractor (MAC) medical director directly, and contact your regional MAC’s Carrier Advisory Committee (CAC) representative. Currently, there is an ENT CAC representative designated to each state within a MAC jurisdiction (15 geographic regions nationwide). Each representative acts as a liaison between Medicare Contractors and state specialty societies. For more information on the CAC representative nomination process, or for local CAC representative contact information, email Health Policy at healthpolicy@entnet.org.
The Academy encourages members to take full advantage of available appeals processes when encountering denied claims. Even in cases where you may feel no progress is made, it is important to exhaust your right to appeal in order to gather all the pertinent information necessary for the Academy to assist you with your issue. Once the recommended efforts have been exhausted, if you still believe a service is being inappropriately denied, the Health Policy team will request a copy of the Explanation of Benefits (EOB) form (with patient HIPAA information redacted) and a copy of the applicable payer policy (this includes denial letters, national or local coverage policies, or any other documentation the payer has provided you during your appeals process), so staff and 3P can determine the root cause of the payer’s denial. 3P will then determine how widespread your specific issue is and whether additional advocacy efforts are required.
If you believe services are being inappropriately denied by a third party payer, or your MAC and have exhausted all appeal options to rectify payment, please contact the health policy team at healthpolicy@entnet.org.
Resources: A NY State Example
A current example of how your state society can assist you comes from the New York State Society of Otolaryngology (NYSSO), which provides assistance to otolaryngologists at the state society level, as part of their member benefits package, and allows NYSSO members in good standing to take advantage of free, unlimited consultation for health insurance coding and billing issues. This service is provided by the Society’s Third Party Consultant, James McNally, who assists otolaryngologists with questions about policy interpretation, use of modifiers, supported diagnosis codes, and non-payment/underpayment of claims for both public and private carriers. In most cases, physicians receive a response within 24 hours.
New York members can contact the NYSSO office at 1-518-439-2020 or meetings@nyssohns.org.