A New Beginning in a Familiar Place
This is a new beginning for me, but I am not a stranger here. I received my medical degree from Louisiana State University School of Medicine in New Orleans and completed my residency at the University of Texas Medical Branch, Galveston, in 1980. After being a community-based practitioner for 33 years, I now have moved from that setting to become a clinical professor at the University of Alabama at Birmingham. I also serve as otolaryngology section chief at the Birmingham VA Medical Center. Within our Academy, I have served in many different roles including board member, coordinator for socioeconomic affairs, and BOG chair. I am also a reviewer for Otolaryngology-Head & Neck Surgery. Throughout the years, I have chaired 3P (Physician Payment Policy Work Group) and our CPT/RVU Committee. On the education side, I have been a member of the Program Advisory Committee, the Instruction Course Advisory Committee, and, until recently, the Education Steering Committee, while chairing Core Otolaryngology Practice Management Education Committee. It is my honor now to serve you this next year as president of the Academy. Within the specialty, I have been a senior examiner for the American Board of Otolaryngology (2008-2012) and on the Editorial Board of the Laryngoscope. I was honored to be named to the AMA CPT Editorial Panel (2004-2008), the body that creates and maintains CPT codes. So, I come to this position with a variety of perspectives, especially in health policy and education, and am certain there are a number of opportunities for us to make a difference together. In my June 2012 official statement as a candidate for AAO-HNS/F president-elect, I stated that our greatest strengths are our strategic planning process and the caliber of Academy leadership. Virtually every significant Academy activity is viewed from the perspective of adherence to this long-range planning that addresses the best interests of our members, and by extension, our patients. This strategic planning is as integral to our operations, as is the identification and mentoring of the next generation of leaders. Our vulnerabilities include the risk of fragmentation, loss of specialty unity, and our relatively small size within the house of medicine. To thrive, we must engage the diversity within the specialty as we identify potential leaders and engage our subspecialty societies to further our advocacy, research and quality, and education activities. So this year I would like to help you, our members, continue to provide quality patient care both by leveraging our strengths and mitigating our weaknesses. Education Our tradition shows that we have been in the forefront of specialty education, but with your help we are adopting new methods of delivering relevant materials to members. For example, the award-winning Academy QTM is helping many prepare for certification on their own schedule. Also note that AAO-HNSF collaboration with the American Board of Otolaryngology on the Fundamentals of Clinical Otolaryngology, (special educational offerings during this year’s Annual Meeting) allowed participants to directly earn maintenance of certification credits. Coordinating education, advocacy, and research within the Academy and with our societies should help avoid duplication and boost productivity, while maintaining the highest standards. We can work to strengthen these activities. Policy and Research Combine for Quality Care The relentless trend of decreased reimbursement coupled with increasing expense and administrative burden continues. Regardless of the fate of the Affordable Care Act, this squeeze is inexorable and will likely result in changes uncoupling reimbursement from the traditional fee-for-service model. I am committed to advancing quality-driven patient care, and enhancing the specialty of otolaryngology-head and neck surgery. This requires evidence-based, health services research, which Academy leadership must help coordinate, foster, and disseminate. Our cross specialty guideline development gives us visibility with primary care physicians, physician assistants, and nurse practitioners as well as consumer groups and ultimately the public. Working with primary care professionals allows us both to strengthen our working relationship and potentially open avenues for investigation for integrated services. The same is true of our RUC and CPT efforts. Through the Ad HOC Payment Model Work Group, we are actively participating and innovating within new models for payment delivery reform. These models are designed to meet the three aims of the National Quality Strategy in the delivery of healthcare services: better care, affordable care, and healthy people and communities. For more detail, visit http://www.entnet.org/practice/paymentreform.cfm. My overarching goal this year is to provide members with as many tools as possible to deal with these challenges and, wherever possible, mitigate unreasonable burdens on our practices and patients.
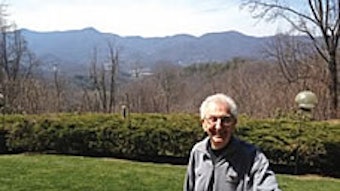
 Richard W. Waguespack, MD AAO-HNS/F President
Richard W. Waguespack, MD AAO-HNS/F PresidentThis is a new beginning for me, but I am not a stranger here.
I received my medical degree from Louisiana State University School of Medicine in New Orleans and completed my residency at the University of Texas Medical Branch, Galveston, in 1980. After being a community-based practitioner for 33 years, I now have moved from that setting to become a clinical professor at the University of Alabama at Birmingham. I also serve as otolaryngology section chief at the Birmingham VA Medical Center.
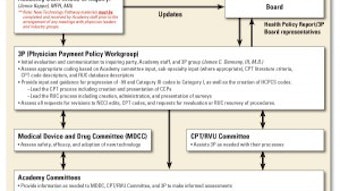
Within our Academy, I have served in many different roles including board member, coordinator for socioeconomic affairs, and BOG chair. I am also a reviewer for Otolaryngology-Head & Neck Surgery. Throughout the years, I have chaired 3P (Physician Payment Policy Work Group) and our CPT/RVU Committee. On the education side, I have been a member of the Program Advisory Committee, the Instruction Course Advisory Committee, and, until recently, the Education Steering Committee, while chairing Core Otolaryngology Practice Management Education Committee. It is my honor now to serve you this next year as president of the Academy.
Within the specialty, I have been a senior examiner for the American Board of Otolaryngology (2008-2012) and on the Editorial Board of the Laryngoscope. I was honored to be named to the AMA CPT Editorial Panel (2004-2008), the body that creates and maintains CPT codes.
So, I come to this position with a variety of perspectives, especially in health policy and education, and am certain there are a number of opportunities for us to make a difference together.
In my June 2012 official statement as a candidate for AAO-HNS/F president-elect, I stated that our greatest strengths are our strategic planning process and the caliber of Academy leadership. Virtually every significant Academy activity is viewed from the perspective of adherence to this long-range planning that addresses the best interests of our members, and by extension, our patients. This strategic planning is as integral to our operations, as is the identification and mentoring of the next generation of leaders.
Our vulnerabilities include the risk of fragmentation, loss of specialty unity, and our relatively small size within the house of medicine. To thrive, we must engage the diversity within the specialty as we identify potential leaders and engage our subspecialty societies to further our advocacy, research and quality, and education activities. So this year I would like to help you, our members, continue to provide quality patient care both by leveraging our strengths and mitigating our weaknesses.
Education
Our tradition shows that we have been in the forefront of specialty education, but with your help we are adopting new methods of delivering relevant materials to members. For example, the award-winning Academy QTM is helping many prepare for certification on their own schedule. Also note that AAO-HNSF collaboration with the American Board of Otolaryngology on the Fundamentals of Clinical Otolaryngology, (special educational offerings during this year’s Annual Meeting) allowed participants to directly earn maintenance of certification credits. Coordinating education, advocacy, and research within the Academy and with our societies should help avoid duplication and boost productivity, while maintaining the highest standards.
We can work to strengthen these activities.
Policy and Research Combine for Quality Care
The relentless trend of decreased reimbursement coupled with increasing expense and administrative burden continues. Regardless of the fate of the Affordable Care Act, this squeeze is inexorable and will likely result in changes uncoupling reimbursement from the traditional fee-for-service model.
I am committed to advancing quality-driven patient care, and enhancing the specialty of otolaryngology-head and neck surgery. This requires evidence-based, health services research, which Academy leadership must help coordinate, foster, and disseminate.
Our cross specialty guideline development gives us visibility with primary care physicians, physician assistants, and nurse practitioners as well as consumer groups and ultimately the public. Working with primary care professionals allows us both to strengthen our working relationship and potentially open avenues for investigation for integrated services. The same is true of our RUC and CPT efforts. Through the Ad HOC Payment Model Work Group, we are actively participating and innovating within new models for payment delivery reform. These models are designed to meet the three aims of the National Quality Strategy in the delivery of healthcare services: better care, affordable care, and healthy people and communities. For more detail, visit http://www.entnet.org/practice/paymentreform.cfm.
My overarching goal this year is to provide members with as many tools as possible to deal with these challenges and, wherever possible, mitigate unreasonable burdens on our practices and patients.