More from November 2014 - Vol. 33 No. 11

Sharon Gnagi, MD
Humanitarian Travel Grant Awardee
Mayo Clinic, AZ
As a medical student at UTMB-Galveston, I promised that one day I would join my mentor, Harold Pine, MD, and then resident, Viet Pham, MD, on their annual mission trip to Vietnam through Resource Exchange International (REI). This year, I had the opportunity to fulfill that promise along with Dayton Young, MD, on Dr. Pine’s 11th trip to Vietnam via scholarships through my residency program at Mayo Clinic Arizona and the AAO-HNS humanitarian travel grant.
The mission of REI is to “build people to build a nation.” With that in mind, we travelled to Ho Chi Minh City and Hanoi, Vietnam, with the primary goal to help educate Vietnamese physicians. Mornings were spent collaborating with local physicians in the operating room, clinic, or hospital rounds while the afternoons were spent in packed auditoriums lecturing to eager Vietnamese residents, medical students, and attending physicians. One of the local favorites was education regarding button batteries, their injuries, and management, as these are becoming increasingly common as the technology of Vietnam advances.
We also had a special educational conference with the Vietnamese residents to focus on leadership and teamwork with special team-building exercises. During this time, a resident shared with me that they make $10 U.S. per month. In addition to teaching me perspective, certainly they taught me many creative ways to manage difficult clinical scenarios with limited resources.
During my time in Vietnam, I visited Tao Dan Park, where each morning it is customary for men to bring their songbirds together. This is an extremely popular custom in Vietnam, and old men sit around the park talking, enjoying coffee, and listening to the birds learn new songs. You see, at home alone, the songbirds will not sing. But each morning at this park, the air is filled with the chirping and cooing of each bird learning new melodies from its neighbors. Each bird leaves with a more beautiful and diverse repertoire. The tragedy is truly the bird not able attend.
As physicians and surgeons, are we not similar to the birds of Tao Dan Park? When we come together, each of us learns new medical information, surgical techniques, and ideas for further research making our medical community better each time we come together. Do we not have a responsibility to share with others what we are so fortunate to know and have easy access to learn? I encourage you to fly around the world and share your songs—you’ll be happy you did, and learn a few songs yourself. Jeremiah C. Tracy, MD
Although many Americans think of Rwanda as a place of violence and starvation, the reality is far different. The nation has moved past the war and genocide of the 1990s and during the last 20 years Rwanda has made great strides. It has the highest literacy rate in central Africa, and incentives to international investors have led to a rapid increase in the nation’s GDP. Despite these advances, the country’s medical system lags behind. At the premier hospital in the nation’s capital, King Faisal Hospital, there is not a single otolaryngologist on staff.
Medical Missions for Children (MMFC) has led mission trips to the town of Gitwe, Rwanda, since 2004. In collaboration with local contacts, this site is now a fully functioning hospital with six general practitioners and two obstetricians. A new medical school (Rwanda’s second) is being built nearby. The connection began when critical care nurse, U.S. citizen, and Rwandan ex-patriot Vianny Ruhumbeza met with Denny Snyder, MD, of MMFC. As Rwanda struggled to rebuild in the late 1990s, Vianny returned home to help manage the family home outside Gitwe. Vianny recognized the need for surgical care in this rural town in the mountains of southwestern Rwanda.
MMFC now runs several trips to Gitwe Hospital each year, providing surgical care to the people in the surrounding region. The team leader, Jagdish Dhingra, MD, has been traveling to Gitwe annually since 2004. In March 2014 I was able to join an annual trip to this site, offering surgical treatment for patients suffering from endemic goiter. Rwanda is an iodine-deficient region. Although an iodinization program is in place, many families live as subsistence farmers and do not typically purchase food from a store. In addition, the local diet is comprised in large part by goitrogens (cassava, potatoes, and cabbage).
As a resident, it was a great exercise for me to think through the diagnostic work-up under absolutely minimal conditions. What aspects are really necessary? This is a far cry from my experience working at an academic medical center in Boston; patients have always been seen previously by endocrinologists, often had multiple FNA procedures, and in some cases even a CT scan to work-up their “neck mass.” In Rwanda we generally had the history and physical exam. Some patients had seen other doctors previously, and may have even had basic thyroid function tests, but most did not. What was the appropriate course of action in order to ensure we were doing the right thing for these patients and not providing second-class care?
On the first day, 60 patients were found to be good surgical candidates. We knew that we had the time, supplies, and stamina to take care of only 30 at most; and new patients continued to show up daily. On days one and two, I was involved only in the operative and post-operative care of patients, and things went quite well. Repetition allowed us to work efficiently and remove five or more huge goiters in a day.
On day three my role was expanded. As usual, we had twice the scheduled number of patients show up. Dr. Dhingra told me, “Go ahead, take a history, examine them, and decide who we should operate on.” This entailed choosing who among many would have surgery, and who would have to return next year.
In many cases, the patients and their families had walked for hours to get to Gitwe. Some had lived with huge goiters affecting their activity and diet for decades. Others were as young as 18 years old and faced the rest of their lives with this condition. To make matters more complicated, Gitwe is a small town. Many of these people knew each other, may even have been distantly related.
I didn’t want to turn people away. I wanted to operate all night long. We discussed the safe allocation of resources. I was forced to acknowledge our inability to help every patient. Those discussions were the most difficult I’ve had in my young career.
In America, we deal with healthcare rationing every day. Will insurance pay for a lab test or an imaging study? How soon can we get this patient on the OR schedule? But as residents we are often sheltered from the actual decision making. On this trip I had my first chance to participate in those difficult decisions. This was an invaluable lesson, both as a physician and as a human being. The most important memory I have from the trip is of squatting outside the hospital in order to be at eye level with a dozen hopeful, seated patients, and having to tell them, through an interpreter, why some would have surgery and some would not. I look forward to returning next year, in order to help those who were turned away. During this year’s Annual Meeting, the Foundation launched an update to one of AAO-HNSF’s most successful and widely used education products: the AcademyQ® Knowledge Assessment app. The app update, which adds 400 additional self-assessment questions to AcademyQ®, is expected to become a favorite member education resource and provide much-needed board exam preparation services to our members and the greater healthcare community alike. The tool is an invaluable resource in ensuring that our physicians remain educated in the most up-to-date treatments and that the highest quality-of-care is being delivered to our patients. Each of the 800 questions contained within AcademyQ® was designed by content experts from our membership and underwent a rigorous peer-review process with the assistance of committee members from the AAO-HNSF’s eight education committees. The app also provides answer rationales for each of these questions along with hyperlinked references to allow for additional reading outside of AcademyQ®.
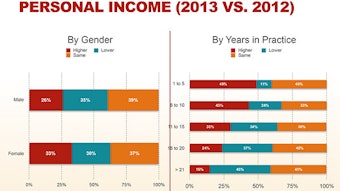
The AAO-HNSF also unveiled a newly-designed android version of the app during this year’s Annual Meeting which will allow AcademyQ® to reach more of our practicing Otolaryngology community than ever before. Both versions of the app, which were designed to work on tablets as well as smartphones, are available as a free download with 10 sample questions which can be upgraded to include either, or both, of the existing 400-question sets for $49.99 each. Since its launch in September 2012, iPhone and iPad users have downloaded the free app 8,100 times and 1,056 individuals have purchased the full app. We hope to continue serving the needs of our users and build upon the success of this product with new question packs released bi-annually as well as additional features, upgrades, and enhancements. Both products can be downloaded directly from a user’s smart phone or tablet by visiting either the Google Play store for Android users or from the iTunes store for Apple users. For more information visit www.entnet.org/academyq. Since 1997, the Academy, through its Health Policy Team, has disseminated a Socioeconomic Survey every three years to all members (excluding military, retirees, and those in training). The survey is an important tool for gathering information on members’practice patterns, the healthcare environment, and future trends in otolaryngology-head and neck surgery. The data collected enables the Academy to help provide members with useful benchmarking tools as well as identifying trends in different practice areas.
This year marked no exception and the Academy is pleased to announce that the results are now available to the membership at-large. To the right is a brief glimpse of some of the results obtained, with a more detailed analysis provided online. Members are encouraged to view the latest data on productivity, revenue, operations, and other practice patterns for the specialty by viewing the full results on the Academy’s Socioeconomic page
at www.entnet.org/content/socioeconomic-data. In 2010, friends of Bobby R. Alford, MD, and many of his past residents came together to honor Dr. Alford’s lifelong contributions to the specialty by establishing an endowment to support an AAO-HNSF CORE grant. This CORE grant will support innovative research in the specialty and help facilitate the career development of young investigators. This mentored research award is intended to lead to improved understanding of the cause or outcomes or to novel treatments for diseases and disorders within the realm of otolaryngology-head and neck surgery.
Bobby R. Alford, MD’s dedication to the specialty of otolaryngology is evidenced by his accomplishments in patient care, education, and research at the department named in his honor at Baylor College of Medicine.
His commitment to education and the training of otolarygologists has led to an amazing legacy. Since 1962, the department Dr. Alford chaired from 1967 to 2010 has trained more than 250 residents and fellows. Many have gone on to have academic positions, including 30 who have become full professors and 16 who have become, or are currently, department chairs.
Dr. Alford believed strongly in the link between research and patient care, as well as the benefits of cooperation between the specialties of the neurosensory systems. He therefore played a significant role in the creation and development of the Neurosensory Center of Houston for The Methodist Hospital and Baylor College of Medicine, which opened in 1977. It was specifically established to promote the educational, research, and clinical objectives and needs of the clinical neurosciences. In this same vein, Dr. Alford also advocated for a close relationship between otolaryngology and audiology and encouraged joint research. Dr. Alford’s own research endeavors resulted in the publication of more than 140 scientific papers, including seminal work in the several areas of otolaryngology.
His efforts to encourage cross-disciplinary research also led to his involvement with U.S. space programs ultimately resulting in the formation of the National Space Biomedical Research Institute established by NASA in 1997, of which he served as its initial CEO. This consortium of 12 institutions continues to lead a national effort to conduct the biomedical research necessary to support long-term human presence, development, and exploration of space and to enhance life on Earth by applying the resulting advances in human knowledge and technology. Rahul K. Shah, MD
George Washington University School of Medicine
Children’s National Medical Center, Washington, DC
We often use this column to speak about patient safety and quality improvement topics that are on the horizon or currently en vogue. One item that is mentioned a lot is the need for measurement. This goes back to the basic business adage that one cannot manage what one cannot measure. Indeed, the patient safety and quality improvement movement has had significant gains and victories in the past decade founded on a strong methodology that includes measurement.
This measurement and evaluations has also started to come to providers. The Joint Commission has a mandatory evaluation tool for providers (physicians, LIPs, etc.) called the On-going Professional Performance Evaluation. Hopefully, every Academy member is aware that the hospitals in which they practice are required to complete an OPPE report on each medical staff member (physician, physician assistant, nurse practitioner, etc.) three times in a two-year cycle. The OPPEs were a relatively new concept a decade ago, however I am quite certain that in the past two-year cycle, every Academy member whom has active privileges should have had an OPPE report on file at their respective medical staff office. The more important question is—have you seen your OPPE report?
Measurement by and of itself may be adequate, but it is compulsory for us to know what is being measured. There is latitude afforded to the individual medical staff offices on how they create the OPPE, what is measured, and the action items from the reports. This freedom allows each medical staff office the ability to customize reports and drive initiatives/change in areas where they feel they would like to focus upon to improve patient safety and quality. For example, a medical staff office may want to focus on hand hygiene compliance, surgical site infections, or re-admission rates. The point being is that Academy members should be aware that such information is collected and maintained by your medical staff office.
What started, perhaps, as a fluff document that a medical staff office would fill out to ensure compliance with the Joint Commission is slowly emerging as a powerful tool with some excellent best practices; the OPPE is increasingly being used for credentialing and in a robust manner. For example, I have heard of some institutions that look at an OPPE to see if there is “over-operation”for specific procedures or diagnoses; or the contrary, if a provider has not performed a specific case in more than two years, they may be denied privileging for that case.
As such, it is compulsory that we own our data. Academy members must be pro-active and reach out to your various medical staffs in the hospitals you practice at to obtain your OPPE report. Traditionally, the Joint Commission recommends that the OPPE report have structure; our organization uses the core competencies such as professionalism, systems-based practice, etc. From here, the recommendation is to have a few key metrics under each category that is provider specific. Examples would be patient satisfaction scores, incomplete operative dictations, etc. What is interesting, an emerging best practice is to list the top five procedures of the specific provider. This enables a chief of staff to immediately scan similar providers to look for variances and outliers.
Such scrutiny and transparency will only serve to benefit our patients so we applaud the OPPE. The caution to our Academy membership is take a few minutes from your busy days and drop by your respective medial staff office and asks to see your OPPE and make sure that the data is accurate and reflects your practice and volumes.
We encourage members to write us with any topic of interest and we will try to research and discuss the issue. Members’ names are published only after they have been contacted directly by Academy staff and have given consent to the use of their names. Please email the Academy at qualityimprovement@entnet.org to engage us in a patient safety and quality discussion that is pertinent to your practice. During the AAO-HNSF 2014 Annual Meeting & OTO EXPOSM in Orlando, FL, Academy members could visit not one, but two, Legislative Advocacy booths to learn more about the Academy’s federal legislative priorities, grassroots initiatives, and political programs. In case you were unable to join us in Orlando, below is a brief overview of what you missed!
Save Our Physicians –In Orlando, AAO-HNS members had the opportunity to sign a petition in support of preserving the term “physician” for MD/DO-trained healthcare providers. Given the introduction of federal legislation (H.R. 5304) that would provide audiologists with “limited license” physician status under the Medicare program, the AAO-HNS is increasing its advocacy efforts to ensure this critical training distinction is preserved. The petition, signed by more than 250 AAO-HNS members, helps our organization send a clear message to Capitol Hill opposing H.R. 5304.
The SRF Expands its Advocacy “Footprint”–Members of the Section for Residents and Fellows-in-Training made an impressive stride in their advocacy efforts during this year’s Annual Meeting. While in Orlando, 84 Residents/Fellows-in-Training became active in the Academy’s Advocacy campaign by contributing to ENT PAC, joining the ENT Advocacy Network, or following Government Affairs on social media. As a result, the SRF increased its overall participation by nearly 80 percent in just a few days. With only a little over a month left in the year, the training program from UC-Irvine is leading the Campaign with 52 points. It’s not too late to get involved! Visit www.entpac.org for additional details.
ENT PAC Success at Annual Meeting–Thanks to the generous support of its Investors, ENT PAC raised more than $19,000 during the AAO-HNSF 2014 Annual Meeting & OTO EXPOSM—far surpassing its fundraising goal.* In addition, the PAC welcomed over 180 new members to the “Investor” ranks, 45 percent of which are resident members of the AAO-HNS.
ENT PAC Investors Enjoy a Night of Jazz–On Monday, September 22, all 2014 ENT PAC Investors were invited to attend the annual PAC “Thank You” reception. This year’s event took place at BB King’s Blues Club in Orlando, FL. The ENT PAC Board of Advisors and staff thank all our 2014 PAC Investors!
Lunch Among Advocacy Leaders–On Monday, September 22, the ENT PAC Board of Advisors hosted the annual Chairman’s Club Luncheon ($1,000+ annual contribution). New for this year, the luncheon also welcomed several of this year’s above-and-beyond “state trackers” and the 2013 SRF Advocacy Involvement Campaign winners, UC-Irvine. During the event, attendees discussed critical healthcare issues with special guest, U.S. Rep. Michael Burgess, MD (R-TX). For more information about the ENT PAC Leadership Clubs or the state trackers program, email govtaffairs@entnet.org.
To receive the latest legislative and political news year round, join our social media networks—“Follow” us on Twitter @AAOHNSGovtAffrs, “Like” us on Facebook, and “Connect” to us on LinkedIn!
*Contributions to ENT PAC are not deductible as charitable contributions for federal income tax purposes. Contributions are voluntary, and all members of the American Academy of Otolaryngology-Head and Neck Surgery have the right to refuse to contribute without reprisal. Federal law prohibits ENT PAC from accepting contributions from foreign nationals. By law, if your contributions are made using a personal check or credit card, ENT PAC may use your contribution only to support candidates in federal elections. All corporate contributions to ENT PAC will be used for educational and administrative fees of ENT PAC, and other activities permissible under federal law. Federal law requires ENT PAC to use its best efforts to collect and report the name, mailing address, occupation, and the name of the employer of individuals whose contributions exceed $200 in a calendar year. ENT PAC is a program of the AAO-HNS which is exempt from federal income tax under section 501 (c) (6) of the Internal Revenue Code.