More from April 2014 - Vol. 33 No. 04
Mark Your CalendarAAO-HNSF Annual Meeting
& OTO Expo 20149/21 – 9/24/2014
Orange County
Convention Center
When the AAO-HNSF 2014 Annual Meeting & OTO EXPOSM opens September 21 in Orlando, we will welcome ENTs from around the globe. Led by International Coordinator James E. Saunders, MD, the International Steering Committee is hard at work developing events tailored especially to international visitors.
New Regional Advisors
New assignments on the committee are Susan R. Cordes, MD, as co-regional advisor for Africa with James L. Netterville, MD; Prof. Marc Remacle, MD, PhD, president, European Federation of Otolaryngology Societies (EUFOS), replacing Prof. Karl Hoermann; and Soha N. Ghossaini, MD, and Ahmed A. H. Soliman, MD, who will step in as co-regional advisors for the Middle East, replacing G. Richard Holt, MD, D-BE, MSE, MPH; and Elizabeth H. Toh, MD, who becomes a regional advisor for Asia-Pacific Rim, with K.J. Lee, MD.
Caucuses and Satellite Meetings
Regional advisors will host caucuses for delegates from Africa, Europe, Latin America, the Middle East, and, for the first time, Asia-Pacific Rim. Other international meetings include an International Women’s Caucus for women leaders from the U.S. and around the world. J. Pablo Stolovitzky, MD, will facilitate the Cumbre de Lideres (Latin American Leaders’ Summit) in Spanish, and Juan Manuel Garcia Gomez, MD, chairs the Panamerican Committee, so there are ample opportunities for Latin American visitors, who constitute the largest international group.
The AAO-HNS-Egyptian satellite meeting, which was a great success at the 2013 meeting in Vancouver, will be expanded to a Middle East Satellite meeting with attendees from Egypt, the Gulf, Lebanon, Saudi Arabia, and many other countries.
Spearheaded by Gregory W. Randolph, MD, and Prof. Bernard G. Fraysse, MD, an AAO-HNS-Francophone satellite meeting is planned for visitors from French-speaking countries.
International Assembly
Last year’s International Assembly was well received, and Orlando will see a robust program for leaders of our International Corresponding Societies (ICS) network. The network now numbers 54 with the newest addition of the Taiwan Society of Otolaryngology. The Assembly will also present the 2014 International Visiting Scholars (IVS), including the Antonio Dela Cruz, MD, Memorial IVS from Latin America; the Nancy L. Snyderman, MD, IVS, awarded to an international woman otolaryngologist; and the Baxiram S. and Kankuben B. Gelot IVS, made possible by the generous support of Raghuvir B. Gelot, MD, and Carolyn Gelot.
Guest Countries and Global Health Symposium
This year, our president, Richard W. Waguespack, MD, will honor four guest countries: Ecuador, the Dominican Republic, Saudi Arabia, and the United Kingdom. The Global Health Symposium will highlight these countries, where regional advisors will introduce experts from these countries to speak on the state of the specialty in their country or region.
International Steering Committee (including regional advisors)
James E. Saunders, MD, coordinator for International Affairs, ex officio committee chair
Nikhil J. Bhatt, MD, development coordinator and chair, International Otolaryngology Committee
Susan R. Cordes, MD, regional advisor for Africa
Terry A. Day, MD, regional advisor for the Caribbean
Ramon A. Franco Jr., MD, regional advisor for Central America
Bernard Gil Fraysse, MD, regional advisor for Francophone Africa
Juan Manuel Garcia Gomez, MD, chair, Panamerican Committee
Soha N. Ghossaini, MD*, regional advisor for the Middle East
G. Richard Holt, MD, D-BE, MSE, MPH, regional advisor for the Middle East
David W. Kennedy, MD, regional advisor for Europe
Chong-Sun Kim, MD, PhD, president of IFOS
K. J. Lee, MD, regional advisor for Asia-Pacific Rim
Eugene N. Myers, MD, FRCS Edin (Hon), regional advisor for the Balkans, Greece, and Turkey
James L. Netterville, MD, regional advisor for Africa
Milan Profant, MD, PhD,
secretary-general IFOS
Gregory W. Randolph, MD, consultant
Marc J. Remacle, MD, PhD*, regional advisor for Europe
Anatoly F. Romanchishen, MD, PhD, DSc, regional advisor for Russia
Hector E. Ruiz, MD, secretary-general, Panamerican Association
Merry E. Sebelik, MD, chair, Humanitarian Efforts Committee
Nancy L. Snyderman, MD, advisor for International Women
Ahmed M. S. Soliman, MD*, regional advisor for the Middle East
J. Pablo Stolovitzky, MD, regional advisor for Latin America
Elizabeth H. Toh, MD*, regional advisor for Asia-Pacific Rim
Mark E. Zafereo, Jr., MD, advisor for International Young Professionals
*Newly appointed
Panamerican Committee
Juan Manuel Garcia Gomez, MD (Colombia), chair
Jacqueline Alvarado Medina, MD (Venezuela)
Hemendra N. Bhatnagar, MD (U.S.)
Emiro E. Caicedo Granados, MD (El Salvador)
Gabriel Calzada, MD (U.S.)
Jose Roberto Castro Montoya, MD (El Salvador)
Alejandra Daza, MD (Venezuela)
Luis A. Macias Fernandez, MD (Mexico)
Hernan Goldsztein, MD (U.S.)
Adam M Klein, MD (U.S.)
Graciela Pepe, MD, PhD (Argentina)
Kevin D. Pereira, MD, MS (ORL) (U.S.)
Steven Daniel Pletcher, MD (U.S.)
Edmund A. Pribitkin, MD (U.S.)
Jonathon O. Russell, MD (U.S.)
Hector M. Santini, MD (U.S.)
Giovana R. Thomas, MD (U.S.)
Tulio A. Valdez, MD (U.S.)
Richard L. Voegels, MD, PhD (Brazil)
International Otolaryngology Committee
Nikhil J. Bhatt, MD, committee chair
Dunia Abdul-Aziz, MD
Sanjay Athavale, MD
Nicolas BuSaba, MD
Juan A. Chiossone Kerdel, MA, MD, FRCS
David W. Clark, MD
W. J. Cornay, III, MD
Arun K. Gadre, MD
Soha N. Ghossaini, MD
Mohammed A. Gomaa, MD
Anthony F. Jahn, MD
Herman A. Jenkins, MD
Ashutosh Kacker, MD
Rajesh S. Kakani, MD
Lily Love, MD
Kevin Christopher McMains, MD
Dinesh C. Mehta, MD
Shri K. Nadig, MD, FRCS, DLO
Mohsen Naraghi, MD
Vaclav Pavelec, MD, PhD
Hassan H. Ramadan, MD, MSc
Anais Rameau, MD
Nikhila M. Raol, MD
Michael J. Rutter, MD, FRACS
Samuel H. Selesnick, MD
Aristides Sismanis, MD
Carl H. Snyderman, MD, MBA
Jesse G. Wardlow, Jr., MD
K. John Yun, MD
Catherine R. Lincoln, CAE, MA (Oxon) 
Ameet K. Grewal, MD
Humanitarian Travel Grant Awardee
With the generosity of the AAO-HNSF Humanitarian Efforts Committee, I was given the opportunity to travel to Southeast Asia to participate in a mission trip focused on otologic surgery. As a current PGY-4 at Georgetown University Hospital, I was honored and excited by the experience. Cambodia is a country severely traumatized by its recent history; it is a nation struggling to find its path after enduring a tumultuous civil war and the perpetration of a vicious genocide on its people. In an effort to eradicate intellectuals, the majority of doctors were executed or exiled from the country. Among the many long-term effects of the Khmer Rouge regime is the lack of physicians and medical access. Considering this history of poverty and violence, coupled with the prevalence of treatable ear disease, patients here benefit greatly from foreign medical missions.
Upon arrival in Phnom Penh in September 2013, I was greeted warmly by the IMPACT Cambodia team. Richard Wagner, MD, founder of Global ENT Outreach (GEO), travels throughout the world teaching and performing otologic surgery. Our team also included Davide Panciera, MD, of Italy, Ineke Wever, MD, of Australia, and Denise Carmer, RN, of Arizona.
We began the week by conducting a clinic in the Preah Ang Duong Hospital and selecting surgical candidates. With the help of Cambodian physicians, we were able to obtain histories from our patients and send them for preoperative audiograms and imaging if needed. After selecting patients, we began operating that afternoon. The strong camaraderie between operating room staff and surgeons overcame whatever language barriers existed, and we operated together into the evening hours. The days that followed only built on that sentiment, proving the bond of operating together surpasses cultural differences.
The Preah Ang Duong Hospital in Phnom Penh is unique in that it caters only to otolaryngological and ophthalmologic surgery. Patients who would have undergone same day surgery in the United States are kept here for a one-week observation on the inpatient unit. Many patients traveled from remote villages to obtain care and remaining in Phnom Penh was the best post-operative option. Routine tympanoplasties and mastoidectomies for chronic middle ear disease were performed under local anesthesia with minimal intravenous sedation. Basic supplies such as ear speculums, gloves, syringes, local anesthetics, operating room drapes, and ear dressings would be helpful to gather prior to a trip. Compared with the United States, operative time was greatly reduced. Without general anesthesia or facial nerve monitoring, we were able to complete 47 cases in five days. The pace and the motivation of every person on our team helped achieve our goal.
I believe a real difference was made in many ways; the patients underwent procedures that allowed them to eradicate middle ear
disease and hopefully restore hearing. Our fellow Cambodian physicians were engaged and learned how to work up these patients and perform surgeries as well. We made a connection with the ENT residents at the hospital and were able to learn from them about the difficulties of training where resources are so limited. The clinic days that generated our cases were busy and crowded, but satisfying. We worked together in a highly effective and efficient manner, with a common goal of helping as many people as we could in that short time.
I highly recommend humanitarian travel to fellow doctors. Seeing how patients are treated in other places in the world allows you to learn and reflect on common practices. I plan on future travel, both as a resident and an attending, to continue to help address the need for service throughout the world. In continuing medical education (CME) it is important that we use evidence-based adult and organizational learning principles to improve the performance and outcomes of our physician learners. In 1970, Educator Malcolm Knowles described “andragogy” as the art and science of helping adults learn. He came up with five assumptions about adult learners that formed the basis for his model. These assumptions are:
Self-concept—being self-directed learners
Experience—accumulated experiences become resources for learning
Readiness to Learn—learning becomes oriented to what is occurring in real life
Orientation to Learning—shifting from subject-centered to problem-centered learning
Motivation—motivation to learn becomes internal in contrast to external rewards
The Foundation considers each of these assumptions as it designs, implements, and evaluates the education opportunities it provides to its members. With this in mind, the 2013 Member Education Needs Assessment Survey asked, as adult learners, what your ideal learning resource would look like. The purpose is to identify the critical features and functionality of an ideal learning platform. Your responses can be summarized into the concept of “On Demand Learning,” with five specific characteristics.
Accessible
You want to have easy access to education and knowledge resources. This includes making sure they are portable and can be found on mobile apps and tablets, as web-based, and in print. Many survey respondents suggested an integration of eLearning and traditional teaching.
Self-Paced
You want to be able to engage in learning at your own pace and time. Education and knowledge resources should provide the opportunity to start and stop the activity as time permits. They need to be available around the clock so physicians can use them on their own schedule. Many indicated they wanted the learning activity to provide feedback on their progress and to assess their learning.
Interactive
Overwhelmingly, you want education and knowledge resources to be engaging and interactive. Many examples were case-based courses, combined lectures and interactive components, hands-on techniques, simulation, practice assessments, and clinical problem solving. Many felt this was the best way not only to gain knowledge but also to master competencies and improve performance.
Easily Digested
This characteristic included easy access, time efficiency, and continuous availability. It also encompassed how the material should be presented such as videos, diagrams and images, algorithms and flow charts, indexing and search functions, and demonstrations.
Customized
Members want the ability to customize their learning experience so that it meets their specific performance gaps and education needs. This includes availability of a variety of offerings, in a variety of formats, addressing all otolaryngology-head and neck specialties. The concept of “personalized learning” would provide a customized education platform specific to each learner.
Another component of the education needs survey addressed the changes in healthcare that would have a significant impact on members’ education needs. The changes include:
Healthcare reform
Government regulation
Requirements of electronic health records
Decreased reimbursements
Focus on electronic education formats with less printed material
Education delivery methods and content
Decreased time to spend on education
Cost of education and knowledge resources
Lastly, we asked your opinions on the need to collaborate with other healthcare groups. The vast majority of respondents agreed that it is very important to partner with other organizations. Suggestions of ways AAO-HNS/F can collaborate include:
Board certification/recertification preparation
Coordination and organization of education resources
Development of guidelines and best practices
Informing members of cutting edge research
Improved patient care and outcomes
More in-depth/specialized information
Joint conferences
Consistency in education messaging and goals
The evolution of healthcare will drive the need for collaboration for AAO-HNS/F. Each of the responses from the member survey will be considered as we develop the next generation of education and knowledge resources.
The Member Education Needs Assessment Survey yielded very valuable feedback and useful information. We have spent the past four months presenting the results to you through a series of Bulletin articles. Much work is underway to implement changes to the Foundation education platform based on the results from the survey. This will be a multi-year effort to build the ideal education platform. Look for future Bulletin articles and other messages describing both incremental and big changes that will impact member engagement and the value placed on the Education Program of the Foundation. The Value-Based Modifier (VBM) Program assesses both quality of care furnished and the cost of care under the Medicare Physician Fee Schedule (MPFS). The Centers for Medicare & Medicaid Services (CMS) are beginning with a phase-in of the VBM in 2015, which will apply to all physicians by January 1, 2017. Implementation of the VBM is based on participation in Physician Quality Reporting System (PQRS). For CY 2013, the VBM applied to groups of physicians with 100 or more eligible professionals (EPs). In 2014, CMS is expanding this to groups with 10 or more.
Groups are defined, for purposes of the VBM, as “a physician (includes doctors of medicine or osteopathy, doctors of dental surgery or dental medicine, doctors of podiatric medicine, doctors of optometry, and chiropractors); OR a practitioner described as (a physical or occupational therapist or qualified SLP; or a qualified audiologist).” To determine what groups have more than 10 providers for purposes of the 2014 VBM reporting period, CMS will query their PECOS system to identify groups and will perform the query 10 days after the close of the PQRS group self-nomination/registration process which occurs in the fall of the year prior to the upcoming reporting period (i.e. occurred in October 2013 for CY 2014 PQRS reporting period). Of note, CMS will not apply the VBM to groups of physicians that are participating in the MSSP program, the Pioneer ACO models, or the Comprehensive Primary Care initiative.
Physician Quality Resource Use Reports
Eligible professionals (EPs) are able to assess their performance, and how they would have performed had the VBM been applied to them in 2013, by downloading their Quality Resource Use Reports (QRURs) from the CMS website at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeedbackProgram/Episode-Costs-and-Medicare-Episode-Grouper.html. These reports will inform physicians how they compare in cost and quality of care to their peers. Visit the Academy website for specifics on obtaining your report at http://bit.ly/entVBPM.
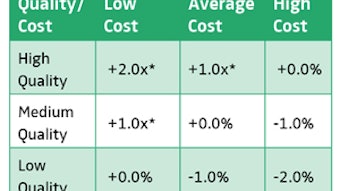
Each group then receives two composite scores (quality and cost), based on the group’s standardized performance (e.g., how far away from the national mean). Group cost measures are adjusted for specialty composition of the group. This approach identifies statistically significant outliers and assigns them to their respective quality and cost tiers.
Attribution of Beneficiaries for Purposes of Assigning Costs
CMS will use the same methodology used for the MSSP ACO program to assign beneficiaries to groups for purposes of the VBM. That is, they will assign beneficiaries based on the delivery of primary care services. For groups that do not provide primary care services, or who have fewer than 20 beneficiaries attributed to them, CMS will assign their cost composite as “average” cost.
For the new 2014 cost measure on Medicare Spending Per Beneficiary (see chart), CMS will attribute the Medicare spending per beneficiary (MSPB) episode solely to the physician group, identified by the TIN, that provided the plurality of Part B services billed during the index hospitalization. CMS will also require physicians to have a minimum of MSPB episodes attributed to them before this measure would be included in their cost composite for calculation of the VBM.
Cost Composites and Benchmarking
CMS will account for specialty mix using a “specialty adjustment” method as it relates to calculating a group’s standardized score for each cost measure and benchmarking against other groups for that performance year. The new specialty adjustment will entail the following:
Creating a national specialty-specific expected costs;
Calculating a specialty-adjusted expected
cost for each group of physicians by weighing the national specialty-specific expected costs by the group’s specialty composition of Part B payments; and
Calculating a specialty-adjusted total per capita cost.
CMS will identify the specialty for each EP based on the specialty they have listed on the largest share of their Part B claims. CMS states that the “specialty adjustment” method accounts for the specialty composition of the group of physicians when making peer group comparisons and creates standardized scores for each cost measure. They also believe this methodology allows the payment modifier to apply to smaller size groups and solo practitioners. CMS states that although the calculations are very detailed, they are transparent and they can provide each group of physicians information on how their costs were benchmarked. CMS believes that the “comparability peer group” method would be less transparent. CMS does not believe it is necessary to delay implementation and will monitor the influence of the specialty adjustment method on physician groups.
Specifics on 2014 VBM requirements are outlined and additional information is available on the Academy website, including a new VBM Fact Sheet, at http://bit.ly/entVBPM.
How Does the Value Modifier Work with PQRS?
How are My Quality and Cost Scores Calculated? CMS recently released the 2014 Inpatient Prospective Payment System final rule, which included a new requirement, commonly referred to as the “2 Midnight Rule.” As members are aware, Medicare has two distinct “Programs” known as Part A (which relates to payment for inpatient services) and Part B (which relates to professional and hospital outpatient services). According to CMS, Medicare beneficiaries having long stays in hospitals as outpatients raised concerns regarding improper payments. Because of such, CMS revised its rule relating to when a patient is deemed “inpatient” versus “outpatient” for payment purposes. Essentially, the rule clarifies that a beneficiary is an inpatient of a hospital if formally admitted via an order by a physician or other qualified practitioner. There are two key principles physicians and qualified practitioners should be aware of regarding the new rule.
First, admission must be “certified” by a physician with an order being a required component of that certification. The order must be written, cited in the medical chart, signed by a physician or other qualified practitioner, and must be completed either prior to admission or at the time of admission. Inpatient status only applies prospectively from the time of formal admission, and the order must specifically state admission as an inpatient. A specific format for the certification and order is not required.
Additionally, certification must include the reason for the inpatient admission, estimated duration of the patient’s stay, and a tentative post-discharge plan. CMS has highlighted some inpatient admission guidelines, which can be viewed at http://www.cms.gov/Medicare-Fee-for-Service-Payment/AcutelnpatientPPS/Downloads/IP-Certification-and-Order-09-05-13.pdf. If a procedure involves one designated by the Hospital Outpatient Prospective Payment System (OPPS) as an inpatient-only procedure then admission and payment under Part A are deemed appropriate. Further, if a physician expects a patient’s stay to transcend two midnights due to a surgical procedure, diagnostic test, or other treatment, and admits the patient based on that expectation, the admission will generally be deemed appropriate for Part A payment purposes. It is important to note, however, CMS has emphasized that there must be “no reasonable possibility that the care could have been adequately provided in an outpatient setting.” It should also be noted that payment will not be deemed inappropriate in circumstances where the expected 2 Midnight stay is cut short, such as by death, transfer, or unexpected rapid improvement.
Second, the new rule distinguishes between the 2 Midnight benchmark and the 2 Midnight presumption. The benchmark serves as guidance for admitting physicians and practitioners and allows Medicare reviewers to identify when an inpatient admission is generally appropriate for coverage and payment. The starting point for determining whether the 2 Midnight benchmark has been met is when the patient begins receiving hospital care on an inpatient basis. In other words, the 2 Midnight clock starts when the beneficiary begins receiving hospital care as an inpatient, assuming admission was reasonable and expected. Conversely, a patient who is receiving care as an outpatient in a hospital operating room and is later formally admitted is not deemed an inpatient during the time spent in the operating room.
CMS cites high improper payment rates for inpatient admissions as the reason for the heightened scrutiny. If a physician cannot make a reasonable prediction, it has been suggested that the patient should not be admitted, but rather, should continue receiving care on an outpatient basis. The actual length of care, patients who are in intensive care, and level of care required are not exceptions to the premise that inpatient regulation is based upon a reasonable and supportable expectation of a 2 Midnight stay.
The 2 Midnight Presumption is guidance for Medicare review contractors when reviewing claims and determining which to review. The presumption is that claims with lengths of stay greater than 2 midnights after formal admission are presumed appropriate for Part A payment. Such stays will not be the focus of review, unless an unwarranted delay or other evidence exists of an abuse of discretion. In other words, the 2 Midnight presumption serves to flag claims that may need additional scrutiny or review, especially in light of CMS’ argument that 36 percent of improper payments are made for inpatient admissions lasting one-day or less. CMS has stated it will continue to monitor all hospitals for intentional or unwarranted delays, abuses of discretion, or any other unnecessary patterns with inpatient services.
The new rules are aimed at reducing long beneficiary stays as outpatients, and clarify if the ordering practitioner expects a beneficiary to stay at least two midnights, they should be admitted as an inpatient. The Health Policy Team will continue to monitor any changes, updates, or alterations to the new rule. To view the complete final rule, visit http://www.entnet.org/Practice/CMS-News.cfm. Members also can email CMS IPPSAdmissions@cms.hhs.gov with any questions regarding admission and/or medical review under the new rule. As members are likely aware, 2014 brings significant changes to the esophagoscopy family of CPT codes. Specifically, the code set was revised to more clearly identify the types of endoscope and approaches used when performing the procedure, as it was agreed that the physician work involved varied depending on these factors. The codes are also grouped by type of anesthesia or sedation used (e.g., general, moderate sedation, or local). Therefore, the new codes are organized based on whether a rigid or flexible endoscope is used, and whether the approach is transoral or transnasal. Given that these procedures are performed by multiple specialties (otolaryngology and gastroenterology), the Academy’s RUC and CPT teams collaborated with several GI societies to revise and present this code set to the AMA RUC, and ultimately, to CMS for valuation in 2014. Of note, the six new rigid transoral codes were valued solely by otolaryngology, whereas several of the flexible transoral and both of the new flexible transnasal codes were valued by both specialties.
Esophagoscopy, Rigid, Transoral
43191–Esophagoscopy, rigid, transoral; diagnostic, including collection of specimen(s) by brushing or washing when performed (separate procedure)(To report transnasal esophagoscopy, see 43197, 43198)
(For diagnostic flexible transoral esophagoscopy, use 43200)
43192–with directed submucosal injection(s), any substance
(For flexible transoral esophagoscopy with directed submucosal injection(s), use 43201)
(For flexible transoral esophagoscopy with injection sclerosis of esophageal varices, use 43204)
(For rigid transoral esophagoscopy with injection sclerosis of esophageal varices, use 43499)
43193–with biopsy, single or multiple
(For flexible transoral esophagoscopy with collection of specimen or biopsy, see 43200, 43202)
43194–with removal of foreign body
(For radiological supervision and interpretation, use 74235)
(For flexible transoral esophagoscopy with removal of foreign body, use 43215)
43195–with balloon dilation (less than 30 mm diameter)
(If imaging guidance is performed, use 74360)
(For esophageal dilation with balloon 30 mm diameter or larger, see 43214, 43233)
(For dilation without endoscopic visualization, see 43450, 43453)
(For flexible transoral esophagoscopy with balloon dilation [less than 30 mm diameter], use 43220)
43196–with insertion of guide wire followed by dilation over guide wire
(For flexible transoral esophagoscopy with insertion of guide wire followed by dilation over guide wire, use 43226)(For radiological supervision and interpretation, use 74360)
Esophagoscopy, Flexible, Transnasal (TNE)
43197–Esophagoscopy, flexible, transnasal; diagnostic, includes collection of specimen(s) by brushing or washing when performed (separate procedure)(Do not report 43197 in conjunction with 31575, 43191, 43192, 43193, 43194, 43195, 43196, 43200-43232, 43235-43259, 92511)
(For transoral esophagoscopy with biopsy or collection of specimen, see 43191, 43193, 43200, 43202)
(Do not report 43197 in conjunction with 31231 unless separate type of endoscope [e.g., rigid endoscope] is used)
43198–with biopsy, single or multiple
(For transoral esophagoscopy with biopsy or collection of specimen, see 43191, 43193, 43200, 43202)
(Do not report 43198 in conjunction with 31575, 43191, 43192, 43193, 43194, 43195, 43196, 43200-43232, 43235-43259, 92511)
(Do not report 43198 in conjunction with 31231 unless separate type of endoscope [e.g., rigid endoscope] is used)
Esophagoscopy, Flexible, Transoral
43200–Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure)
(For diagnostic rigid transoral esophagoscopy, use 43191)
(For diagnostic flexible transnasal esophagoscopy, use 43197)
(For diagnostic upper gastrointestinal endoscopy, use 43235)
43201–with directed submucosal injection(s), any substance
(For rigid transoral esophagoscopy with directed submucosal injection[s], use 43192)
(For flexible transoral esophagoscopy with injection sclerosis of esophageal varices, use 43204)
(For rigid transoral esophagoscopy with injection sclerosis of esophageal varices, use 43499)
(Do not report 43201 in conjunction with 43211, 43204, 43227)
43202–with biopsy, single or multiple
(For rigid transoral esophagoscopy with biopsy, use 43193)
(For flexible transnasal esophagoscopy with biopsy, use 43198)
(For upper gastrointestinal endoscopy with biopsy or collection of specimen, see 43235, 43239)
43215–with removal of foreign body
(For radiological supervision and interpretation, use 74235)
(For rigid transoral esophagoscopy with removal of foreign body, use 43194)
(For upper gastrointestinal endoscopy with removal of foreign body, use 43247)
43220–with transendoscopic balloon dilation (less than 30 mm diameter)
(For rigid transoral esophagoscopy with balloon dilation [less than 30 mm diameter], use 43195
(If imaging guidance is performed, use 74360)
(For esophageal dilation with balloon 30 mm diameter or larger, use 43214)
(For dilation without endoscopic visualization, see 43450, 43453)
(Do not report 43220 in conjunction with 43212, 43226, 43229)
43226–with insertion of guide wire followed by passage of dilator(s) over guide wire
(For radiological supervision and interpretation, use 74360)
(For rigid transoral esophagoscopy with insertion of guide wire followed by dilation over guide wire, use 43196)
(Do not report 43226 in conjunction with 43212, 43229)
(For additional Flexible, transoral codes see 43200-43233 in the 2014 CPT® Book). Rahul K. Shah, MD
George Washington University School
of Medicine
Children’s National Medical Center, Washington, DC
I am rarely dogmatic, but I implore our Academy membership to visit http://www.nejm.org/doi/full/10.1056/NEJMp1314965 and take 15 minutes to read an article from the New England Journal of Medicine about the Choosing Wisely campaign.1 The authors begin with a noble goal of elevating the status of the Choosing Wisely campaign in the Perspective column of the journal. In the introductory paragraphs, they accurately note how the campaign is different from other initiatives in that, “The message, the messenger, and the method are key features of this stewardship initiative.”1 The Choosing Wisely campaign has been embraced and applauded by medical societies as it asks providers to define those services that are low-value services, “emphasizing individual patients’ needs as the top priority, preserving the preeminence of physician judgment, patient choice, and the therapeutic dyad. Doctors and their societies, not payers, develop the lists.”1
Unfortunately, the article continues with the theme that by empowering physicians and our respective societies to create a list of low-value services, that we as practitioners are inherently self-serving and have political motives driven by a desire to optimize our own reimbursement. Aided by Academy member Richard M. Rosenfeld, MD, MPH, and our EVP and CEO, David R. Nielsen, MD, we immediately wrote a letter to the editor at the New England Journal of Medicine. Whether this is published or not is beyond the point; what is imperative is that Academy members understand that we interpreted and responded to the Choosing Wisely campaign as we were instructed. The goal of Choosing Wisely is to aid patients in interpreting medical advice and to curb overutilization of those services that physicians and societies consider as low-value. As such, many societies provided examples of low-value services that broadly influence a significant number of patients. The authors inaccurately assert that these societies listed their low-value services to preserve our own economic interests while directing attention to other specialties. This is quite a perverse argument that is not justified by data, rather by simply showing the lists of the societies and claiming that they were created by self-interested societies.
It is unfortunate and obvious that the authors did not seek out an opportunity to speak with or read our explanation from the societies to understand our methodology, which has been documented.2 The article calls out the American Academy of Orthopaedic Surgeons and other societies, including ours: “The American Academy of Otolaryngology—Head and Neck Surgery, for example, lists three imaging tests and two uses of antibiotics but no procedures, despite decades of literature on wide variation and overuse of tonsillectomy and tympanostomy tube placement.”1 The inherent conflict with this assertion juxtaposed to the rest of their article is frustrating—our Academy approached the Choosing Wisely list in a democratic manner, asking the various subspecialties to identify low-value services that they see and experience with their patients.
Indeed, if we had focused solely on procedures that are low-value services, then we would not have the largest influence that we believe we can by looking at antibiotic and radiologic overuse—items that influence various disciplines of providers—family practitioners, internists, emergency physicians, pediatricians, etc. We anticipate in further versions of the Choosing Wisely campaign we will use our guidelines and other evidence-based medicine to identify such low-value services.
I am going to make an unfounded assertion that is simply a personal observance—we all think that some other society besides our own—generalists’ or specialists’—are part of the problem of overuse. Hence, we are quick to assert that such “calling the other out” was motivated by economic self-interest rather than what it is—an attempt to genuinely help patients on a broad level.
I applaud our executive leadership and Boards of the Academy for leading the surgical specialties in the Choosing Wisely campaign; we are fortunate to continue to be national leaders in improving the care of our patients and we eagerly look forward to participating in this unique endeavor to identify more opportunities for healthcare as a whole to influence the broadest proportion of patients—one low-value service at a time.
We encourage members to write us with any topic of interest and we will try to research and discuss the issue. Members’ names are published only after they have been contacted directly by Academy staff and have given consent to the use of their names. Please email the Academy at qualityimprovement@entnet.org to engage us in a patient safety and quality discussion that is pertinent to your practice.
References
Morden NE, Colla CH, Sequist TD, Rosenthal MB. Choosing Wisely—The Politics and Economics of Labeling Low-Value Services. N Engl J Med. 2014 Feb13;370(7):589-592.
Robertson PJ, Brereton JM, Roberson DW, Shah RK, Nielsen DR. Choosing Wisely: our list.
Otolaryngol Head Neck Surg. 2013 Apr;148(4):534-6.