More from February 2014 – Vol. 33 No.02

Anya J. Miller, MD
Humanitarian Grant Awardee,
Resident, Henry Ford Hospital
Royal Oak, MI
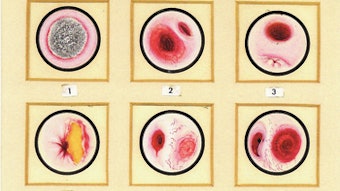
Last September, I traveled with a team from Henry Ford Hospital and the University of Michigan to Migori, Kenya, with Kenya Relief. Under the supervision of Lamont R. Jones, MD, and Greg Basura, MD, PhD, we performed otologic surgery at the Brase Clinic. With the assistance of local nurses, scrub techs, and nurse practitioners, we were able to perform surgeries including hemithyroidectomies, tympanoplasties, cleft lips, and various lumps and bumps.
Although we operated out of a clinic and not a hospital, our patients were able to stay overnight for observation due to the support of local nurses. Despite the occasional fly in the operating room, we enjoyed many amenities such as air conditioning, OR tables that moved up and down, operating microscopes, and Neptune suction machines, to name a few. In fact, after touring the local district hospital, our clinic appeared much better equipped thanks to many generous donations throughout the years. Supplementing with some supplies from home such as an ear tray and LED headlights, we were able to safely provide surgical care to the people.
The majority of the surgical patients who arrived for ENT evaluation were women with goiters. While we were able to alleviate much of the compression and cosmetic deformity with a hemithyroidectomy, we were not able to provide them with a real long-term solution. For smaller goiters, we prescribed iodine drops and education on iodized salt. It was unfortunate that we had not brought with us any iodine drops to dispense to the patients, so how many people were actually able to get the medication is uncertain.
While I do believe our team made a difference and patients were happy to have the surgery, multiple ENT teams arrive at the Brase Clinic each year and perform many surgeries for goiters. Despite this, the patients lined up with goiters are endless each time. It seems that the people in Kenya could benefit from ENT mission groups joining efforts with public health specialists. Given all the resources invested in taking a team to Kenya, a multidisciplinary approach to this issue could be both cost effective and provide a more substantial benefit to the local people. Without this or a similar effort, it seems inevitable that the lines of people waiting to have their goiters removed will continue to be lengthy.
While we were there to serve the people of Kenya, from a resident’s perspective, there was much personal benefit derived from this experience as well. I was able to give my undivided attention to each surgical case without pagers going off, heading off to complete other clinical duties, or anything else that might draw my attention away from the case at hand. We also performed similar cases often, so I was able to learn from each case and improve on those skills without having days or weeks between cases to forget what I had learned. Having consistency in attendings also meant that I could reliably anticipate the next move, which also seemed to accelerate my learning.
Medical missions are in general a huge undertaking for everyone involved, but patients are universally thankful and resident benefit is priceless. Because time and money committed to this endeavor is great, each mission group should look at the needs of the particular area and try to tailor their mission accordingly to maximize impact. Many thanks to the AAO-HNSF Humanitarian Efforts Committee for its grant that made my participation possible.
Kenya Relief Brase Clinic
P.O. Box 1078
Suna, Migori
Kenya, Africa 40400
Contact:
Dominic, Clinical Officer
011-254-724-777-048
Keptembwa@yahoo.com Always seeking to improve education for members, the AAO-HNS Foundation embarked on a year-long education needs assessment in 2013. The recent member-wide survey provided enlightening and actionable data regarding member’s perceptions of our education offerings. The five central themes that emerged were described in the January 2014 Bulletin: member awareness, engagement, and value; existing education products; technology and learning styles; collaboration; and ideal education platform. In the first of the series, this article presents findings from the survey regarding member awareness, engagement, and value in Foundation education and knowledge resources.
Member Awareness
Though a vast majority of members showed familiarity with the Annual Meeting & OTO EXPOSM and the Home Study Course, the familiarity did not extend to the 15-plus other knowledge products provided by the foundation. More than half of members are not aware that the Foundation offers free education resources such as online courses and lectures, COOL, COCLIA, and eBooks as a member benefit. More than one-third of the members were unable to distinguish between free education resources and those that are fee-based.
Whether you are a long-time member or relatively new to the specialty, you may also be missing out on valuable resources. Take a look at the 2014 Educational Opportunities at www.entnet.org/EducationAndResearch/upload/2014_AcademyU_EduOpps_Final_Optimized.pdf or visit www.entnet.org/academyU to check your own knowledge of AAO-HNSF’s education and knowledge resources.
Member Engagement
The survey provided some positive news about member engagement in education, but also showed some opportunity for improvement—particularly for longer-term members. According to the survey, two-thirds of the respondent’s current continuing education needs are fulfilled by the Foundation. Half of those completing the survey plan to continue to or increase their engagement in education with the Foundation during the next three years. Newer members are particularly heavy users, indicating that they have accessed four or more education resources in the past three years. While this is all great news, we also learned that nearly one-third of long-term members have not used any Foundation education resources in the past three years. While one-third of members receive all of their education from the Foundation, many turn to other organizations as well. An additional one-third of respondents indicate that they rely on one other organization in addition to the AAO-HNSF for their education. Members list a variety of organizations they use for continuing education purposes with other otolaryngology specialty organizations making up the majority of other resources.
Value
The perceived value of the Foundation’s education content is high among long-time members, but newer members rate the value significantly lower. This decline in value between long-term and short-term members may indicate there are gaps in quality content, learning formats, delivery of information, or some combination of all three in the minds of the short-term members.
In general, the Foundation has a positive reputation among its members in terms of education. More than half of members rate the value of education resources as very good and also indicate they are very likely to recommend them to others. However, both value and likelihood to recommend is lowest for younger members.
The most common reasons the Foundation education resources offer better value than other organizations include:
Education content is more relevant to area of practice or interests
Wider variety of topics covered
Greater quantity of offerings / resources
More advanced / in-depth content
Accessibility / navigation / organization
More online offerings
Current / cutting edge
The most common reasons the Foundation education resources offer worse value than other organizations include:
Education content is less relevant to my area of practice or interests
Expense of education products
Content is too broad / too focused on generalists
Fewer offerings available
Poor accessibility
Not as current or up-to-date
Members do not see the Foundation as “providing one-stop-shopping” for all education needs.” Significant work will be required on the part of our education leadership to determine whether that goal is achievable, and if so, how to raise the bar to that level.
The relationship between member awareness, engagement, and value of education and knowledge resources will be an overarching measure of success as we work to build a better education platform for members. Through improving the perceived value of its offerings, the Foundation will secure its spot as the primary source for otolaryngology education. Since 1997, the Academy, through its Health Policy Team, has disseminated a Socioeconomic Survey every three years to all members (excluding military, retirees, and those in training). The survey is an important tool for gathering information on members’ practice patterns, the healthcare environment, and future trends in otolaryngology-head and neck surgery. This data enables the Academy to provide members with useful benchmarking tools.
The survey is the most recognized otolaryngology-specific member survey available and allows the Academy to identify key issues and policies affecting members, particularly as they relate to practice productivity, revenue, and operations. The Academy encourages all eligible members to get involved and lend their voice to this important survey.
Members will be able to complete the online survey February 18-March 31 after receiving a unique link to their designated email address.
Your participation is essential for strong, statistically meaningful results. The published aggregate results serve as an asset for members when measuring themselves against their peers.
Aggregate results will be published by an independent research firm in the November Bulletin, and will be on display at the 2014 Annual Meeting in Orlando, Florida, September 21-24. For more information on the AAO-HNS Socioeconomic Survey, please email the Health Policy Team at healthpolicy@entnet.org. In an effort to provide clarification about the differences among the quality knowledge products the Academy provides, the Ad Hoc Payment Model Workgroup has summarized the products including the Clinical Practice Guidelines (CPG) and Clinical Consensus Statements (CCS)s as compared to other Academy documents such as Clinical Indicators (CI)s, and Position Statements (PS)s, providing members with descriptions of the documents and how to use them. These documents can be viewed at http://www.entnet.org/Practice/loader.cfm?csModule=security/getfile&pageID=175934.
The Health Policy unit and the Physician Payment Policy (3P) Workgroup oversee the process for the development, review, and update of the position statements. Below are more details about the definition of a position statement, the process to create a position statement, and a summary of the recent review of all position statements.
Position Statements Defined
A position statement (formerly known as “policy statement”) is used to designate a statement, policy, or declaration of the AmericanAcademy of Otolaryngology—Head and Neck Surgery, and Foundation (AAO-HNS/F) on a particular topic or topics. Statements are created to formalize the AAO-HNS/F position on a clinical procedure or medical service with third party payers, for use in state and federal regulatory or advocacy efforts, or to clarify the AAO-HNS/F approval or disapproval of certain practices in medicine.
Creating a Position Statement
Position statements are generated from within AAO-HNS/F committees. However, an individual member may request consideration of a topic for position statement development. If a member would like to propose the Academy consider developing a position statement on a particular topic, or revisions to an existing position statement, the details about the topic and concerns should be emailed to healthpolicy@entnet.org. The next steps in the process include:
Academy staff will route the request to the Academy’s 3P workgroup for review and determination of which committee(s) should receive the draft position statement for consideration.
The Chair of the committee(s) receives the request, examines the need for a statement, and works to draft the necessary position statement language.
Academy staff will present it to 3P for review. If 3P has questions related to the draft position statements, they are relayed back to the committee(s) for further clarification, and then sent back to 3P for review.
The position statement is then submitted to the Board of Directors (BOD) for review and approval. If the Executive Committee (EC) or BOD has any requests for clarification, they ask 3P, or related committee, to re-review and re-submit. Once the EC has approved, the request for a new or revised position statement is submitted to the Board of Directors during their biennial meetings for final approval. After that, the position statement is posted to the website. The same process is followed for any updates to the position statements.
2012–2013 Review Position Statements
3P and the Health Policy team are committed to ensuring the position statements are updated and useful for members.
In August 2012, a process was initiated to review all of the position statements since they had not been reviewed for several years. At the commencement of the review process, there were 74 position statements. The position statement update process was reviewed and approved by the 3P.
3P initially divided the position statements into three tiers for three separate rounds of review during the course of a year (September 2012-September 2013) taking multiple factors into account for priority including how outdated each statement was, concurrent ongoing research and guideline development, and utilization of each.
After prioritization, 3P assigned each of the statements to the clinical committee(s) of corresponding expertise for review and update. The committee(s) then made recommendations to reaffirm, revise, or delete assigned Position Statements.
Round 3: In September 2013, after an extensive third-round review process by AAO-HNS committees, the EC, and Board of Directors, the Academy reaffirmed eight position statements and revised 10. The third-round updates can be found on the Academy website at www.bit.ly/PositionStatements.
Several existing and new position statements are undergoing further committee review in an effort to reach a consensus on suitable language prior to Board approval.
The Academy currently reviews all position statements on a rolling four-year basis. The first round of review began in September 2012 and we continue to ensure that Position Statement content is up to date. Rahul K. Shah, MD
George Washington University School of Medicine
Children’s National Medical Center, Washington, DC
My hospital is making me see more patients and is going to penalize me financially for not achieving a patient satisfaction goal of more than 90 percent where patients rate me as “very good”! —AAO-HNS member
The email I received from the Academy member above succinctly juxtaposes the competing demands that clinicians are currently facing: increasing volumes (in the face of declining reimbursement) and improving patient satisfaction. Many AAO-HNS members have implored me to write this month’s column to demonstrate that this dual aim is simply not possible.
Since when did a monthly column dedicated to improving safety, quality, and outcomes for our patients start discussing the satisfaction of our patients? As you may have noticed, over the past five years, this column has tried to keep AAO-HNS members abreast of the latest trends in patient safety and quality improvement. We have discussed myriad topics such as zones of risk, pitfalls, strategies to ameliorate problems, reporting systems. Recently, probably in the last 18 months, we have started discussing the issue of patient satisfaction and how payers and others are using this as a pure quality measure and linking reimbursement and even at-risk compensation to ensure our patient’s experiences are the “top box.”
The literature certainly supports that an optimized patient experience drives overall quality and is a surrogate for safety within an organization. However, operationalizing this is difficult.
For example, I could guarantee that I would run/manage the safest and most efficient operating room in the world. It is easy to do this: I would simply operate on one patient a month. We would ensure that we spent millions of dollars and resources to keep that patient safe. If you ask me to do this for a thousand patients a month, it becomes difficult. Similarly, as the AAO-HNS member writes above, it is becoming difficult for physicians to increase their clinical volumes to achieve Relative Value Unit (RVU) targets while optimizing patient satisfaction. On many levels the paradox becomes apparent—the waiting room is swamped, your staff is exhausted, your phone line pick-up times are extended, etc.
Elements Are Not Equal
The problem is that external forces are driving hospitals to include the experience of care in their metrics and eventually will tie this to reimbursement. Organizational scorecards have started emphasizing and reporting on patient experience and satisfaction. The end result of such is that these organizational priorities have trickled down to the providers. The stress that organizations are feeling from external agencies is now being transferred to the providers and the competing demands emerge.
I am secretly worried that piggybacking patient satisfaction to quality and safety will de facto erode the huge gains the industry has made in improving the overall outcomes of our patients. I have had the pleasure of hearing James Merlino, MD, the chief experience officer of the Cleveland Clinic, speak many times. One of his excellent analogies on these competing demands uses the airline industry as an example. He states that when we fly, our absolute priority is to not crash (safety), we really want to take-off and arrive on time (quality/ efficiency), and if the first two criteria are met, it would be great to have a nice experience (satisfaction). How does this relate to the hospital and how do we prioritize patient safety, quality, and satisfaction? We can use Dr. Merlino’s airline analogy to help us prioritize these demands in our realms of care.
I wish I had an easy answer or a crystal ball to assuage our AAO-HNS members’ concerns. What I can guarantee is that for the short-term, there is no solution in sight and I eagerly look toward our exceptionally intelligent, passionate, and motivated membership for innovative solutions to this apparent paradox.
We encourage members to write us with any topic of interest and we will try to research and discuss. Members’ names are published only after they have been contacted directly by Academy staff and have given consent. Please email the Academy at qualityimprovement@ entnet.org to engage us in a patient safety and quality discussion pertinent to your practice. James C. Denneny III, MD
Coordinator for Socioeconomic Affairs
Jane T. Dillon, MD
Coordinator for Practice Affairs and Co-chairs of 3P
The Physician Payment Policy Workgroup (3P), co-chaired by James C. Denneny III, MD, and Jane T. Dillon, MD, is the senior advisory body to Academy leadership and staff on issues related to socioeconomic advocacy, regulatory activity, coding or reimbursement, and practice services or management. 3P and the Health Policy staff were busy in the last quarter of 2013 with a continued high level of activity, constant emails, and monthly calls, working diligently and tirelessly on behalf of all members.
Key 3P Accomplishments Included: Face-to-Face Meeting with CMS/CMMI Representatives in November 2013
In early November, Academy leaders James C. Denneny, III, MD, Lisa E. Ishii, MD, MHS, (coordinator-elect for Research and Quality Improvement) and David Nielsen, MD, along with Health Policy and Research/Quality Improvement staff, Jean Brereton, MBA, senior director, Research, Quality and Health Policy, and Jenna Kappel, MPH, MA, director, Health Policy, met with Patrick Conway, MD, chief medical officer for Centers for Medicare & Medicaid Services and acting director for Center for Medicare & Medicaid Innovation (CMMI), along with other top officials at CMS to discuss payment reform efforts and the need for development of additional clinical quality measures to ensure successful participation in the PQRS and Value Based Modifier programs by otolaryngologists. The Academy representatives inquired as to why five of the nine sinusitis measures were not accepted within the 2014 proposed fee schedule, and outlined our continued concerns regarding CMS’ proposed Outpatient Prospective Payment System cap policy, which, if finalized in 2014, would reduce practice expense relative value units for 13 otolaryngology services when performed in the office setting. This meeting was yet another effort by the Academy to ensure CMS understands the critical role otolaryngologists play in the healthcare system and the influence these programs and policies have on our specialty.
Direct Impact: Our meeting with Dr. Conway was instrumental in acceptance of four adult sinusitis measures for 2014 PQRS reporting. Continued dialogue also maintains the Academy’s high-level visibility with CMS. As a result of numerous advocacy efforts, including these face-to-face meetings, and comment letters, CMS decided not to move forward with the OPPS cap policy and finalized the four adult sinusitis measures for PQRS reporting in 2014. For more details on the Medicare Physician Fee Schedule final rule’s influence on otolaryngology, see page 31.
Regulatory Issues: Academy Advocates on Behalf of Members
Meaningful Use Stage 3
In November, the Academy submitted a comment letter to CMS regarding Proposed Clinical Quality Measures (CQMs) for Use in Stage 3 of the EHR Meaningful Use Incentive Program. Specifically, the proposed Stage 3 measure on Overuse of Diagnostic Imaging for Uncomplicated Headache. The letter also reiterated the Academy’s concerns regarding Stage 2 timing requirements and Stage 3 thresholds and penalties. Input was based on feedback from the Imaging Committee, PSQI, and 3P.
Colorado Clean Claims Act
The Academy has been active in providing comments to the Colorado Clean Claims Act Task Force, an effort to develop a standardized set of payment rules and claim edits to be used by payers and healthcare providers. This is being closely monitored as it could be used in many other parts of the nation. In the summer, we submitted a formal letter on the first round of rules released for comment. These comments were reviewed and vetted through the CPT team, Richard Waguespack, MD, Bradley F. Marple, MD, and Lawrence M. Simon, MD. During the second round of review, the task force liaison reached out to the Academy directly, seeking our input on a few of the rules, and we provided input on the multiple procedure payment rule and the modifier -50 draft rule. Finally, the task force liaison sent us an early preview of the third round proposed rule on multiple endoscopies, which the CPT team reviewed in October and submitted comment on.
ICD-10
Also in November, the Academy submitted comments to the Centers for Disease Control and Prevention regarding the new ICD-10 Codes for Unilateral Hearing Loss in support of the Conductive and Sensorineural Hearing Loss proposal presented during the ICD-10-CM/PCS Coordination and Maintenance Committee Meeting on September 18, 2013. The comments oppose the removal of references of contra-laterality and instead state that the codes are unilateral and retain language referencing which ear the diagnosis relates to. This will facilitate the fact that different types of hearing loss conditions can exist in each ear.
RUC and CPT Update
The Academy is surveying new CPT code 4319X in preparation for the January 2014 AMA Relative Value Scale Update Committee (RUC) meeting. After only a week and a half, the Academy obtained an impressive 146 responses. The minimum requirement by AMA is 30 surveys so this response rate is excellent and is helpful to the Academy’s RUC team, who must base the recommendations for relative value units (RVUs) on the data received. The survey closed early December and was sent to our practicing members specializing in head and neck and laryngology/bronchoesophagology with the support/assistance of AHNS, ALA, and ABEA. Many thanks to the physician leadership of these subspecialties who made the large survey response possible.
AMA CPT/RBVS Symposium At the AMA CPT/RBVS Symposium in Chicago, Dr. Waguespack presented on new, and modified, CPT codes for otolaryngology for 2014, including flexible and rigid transnasal esophagoscopy (otherwise known as TNE) and chemodenervation of the larynx for spasmodic dysphonia, which were RUC surveyed by the Academy. Jenna Minton, Esq, senior manager, Health Policy, also represented the Academy at this meeting.
Academy Releases New CPT for ENT Coding Guidance
You may have noticed that your 2014 CPT Code Books include several modifications and additions to CPT codes used to report otolaryngology services. To assist members in understanding these changes and achieving correct coding, the Academy has revised our CPT for ENT articles on CPT 69210 Removal Impacted Cerumen and CPT 64617 Chemodenervation of Larynx (formerly reported by CPT 64613). These articles can be found in our Coding Corner of the website at www.bit.ly/CPT4ENT.
Academy Collaborates with UHC on Septoplasty Coverage Policy and Provides Feedback on Premier Designation Program
In November, Academy physician leaders, Drs. James Denneny and Richard M. Rosenfeld, MD, MPH participated in a conference call with United Healthcare National Medical Director Richard Justman, MD, and other physician leaders at UHC, to discuss and provide feedback on United’s Premier Designation program. This program recognizes physicians who meet certain cost/quality parameters and highlights them with a “Premier” designation in the UHC physician networks. During the call, we were able to get confirmation from UHC leadership to work in partnership with otolaryngology to develop future models for reimbursement.
The Academy has also been collaborating with UHC to provide comments regarding their Rhinoplasty, Septoplasty, Vestibular Stenosis policy and are working with them to address issues we’ve continued to hear from members related to receiving a septoplasty review that was approved prior to surgery, but denied coverage following surgery. UHC is working to correct these issues. Also, the Academy is providing UHC with recommendations about patient criteria for septoplasty for UHC to consider including in their coverage policy.
New HP Team Member
The Health Policy team welcomes Danielle Jarchow, Esq, to the staff as a health policy analyst. Danielle comes from a family of otolaryngology-head and neck surgeons with her father and sister, who practice in academic and private practice, members of the Academy.
“HP Update” Archives
Missed the last edition of the “HP Update”? Access the monthly newsletter: http://www.entnet.org/Practice/HP-Update.cfm.
For questions on the above Health Policy issues, please send an email to HealthPolicy@entnet.org. Special thanks to our investors for their commitment to advancing the specialty!
Chairman’s Club
Investment of $1,000+ Annually
Nikhil J. Bhatt, MD
C. Y. Joseph Chang, MD
Susan R. Cordes, MD
Stephen P. Cragle, MD
Agnes Czibulka, MD
Scott A. Dempewolf, MD
Lee D. Eisenberg, MD, MPH
Wayne B. Eisman, MD
Cameron D. Godfrey, MD
Steven D. Horwitz, MD
Paul M. Imber, DO
Stacey L. Ishman, MD, MPH
Alice L. Kuntz, MD
Steven B. Levine, MD
J. Scott Magnuson, MD
Theodore P. Mason, MD
Samantha Marie Mucha, MD
Nathan E. Nachlas, MD
David R. Nielsen, MD
Robert Puchalski, MD
R. Arturo Roa, MD
Richard M. Rosenfeld, MD, MPH
Michael D. Seidman, MD
Gavin Setzen, MD
Adam M. Shapiro, MD
Paul F. Shea, MD
Lawrence M. Simon, MD
William H. Slattery III, MD
Gangadhar Srikumar Sreepada, MD
Oscar A. Tamez, MD
John H. Taylor, MD
Ken Yanagisawa, MD
Kathleen Yaremchuk, MD, MSA
Jay S. Youngerman, MD
Resident Chairman’s Club
Investment of $500+ Annually
Nathan Deckard, MD
Timothy O’Brien, MD
Capitol Club
Investment of $535+ Annually
Peter J. Abramson, MD
Michael A. Alexiou, MD
Anna Aronzon, MD
Jonathan E. Aviv, MD
Dole P. Baker, Jr., MD
Paul A. Bell, MD
Drupad Bhatt, MD
Bradley B. Block, MD
Marcella R. Bothwell, MD
Kevin Braat, MD
Richard J. Brauer, MD
Robin M. Brody, MD
Henry Frederick Butehorn III, MD
Mark E. Carney, MD
John A. Cece, MD
Sujana S. Chandrasekhar, MD
Won-Taek Choe, MD
Jason P. Cohen, MD
Tahl Ya’ari Colen, MD
Jeffrey N. Cousin, MD
Jeffrey J. Cunningham, MD
Robert J. Cusumano, MD
Richard DeMaio, MD
Elizabeth A. Dinces, MD
Gary S. Fishman, MD
Randy J. Folker, MD
Jeffrey B. Ginsburg, MD
David A. Godin, MD
Steven M. Gold, MD
Michael S. Goldrich, MD
Michael A. Gordon, MD
Robert P. Green, MD
Karen L. Hermansen, MD
Michael R. Holtel, MD
John J. Huang, MD
Madan N. Kandula, MD
Matthew J. Kates, MD
Natasha F. Keenan, MD
Ronald H. Kirkland, MD, MBA
Timothy D. Knudsen, MD
Mitchell T. Kolker, MD
Russell W. H. Kridel, MD
Ronald B. Kuppersmith, MD, MBA
Brian L. Lebovitz, MD
Marc J. Levine, MD
Guy Lin, MD
Pei S. Lin, MD
Scott B. Markowitz, MD
Michael G. Mendelsohn, MD
Charles Mixson, MD
Alice H. Morgan, MD, PhD
Eric A. Munzer, DO
James L. Netterville, MD
Timothy O’Brien, MD
Rick Odland, MD, PhD
Sheldon Palgon, MD
Ira D. Papel, MD
Rami N. Payman, MD
Spencer C. Payne, MD
George A. Pazos, MD
David Poetker, MD, MA
Liana Puscas, MD
Jay S. Rechtweg, MD
Andrew J. Reid, MD
Edward B. Rhee, MD
Eric Roffman, MD
Steven H. Sacks, MD
Zarina Sayeed, MD
B. Todd Schaeffer, MD
Daniel A. Scher, MD
Scott R. Schoem, MD
Jerry M. Schreibstein, MD
Charles M. Schultz, MD
Merry E. Sebelik, MD
Elizabeth A. Shaw, MD
Michael R. Shohet, MD
Joseph R. Spiegel, MD
J. Pablo Stolovitzky, MD
Jerome O. Sugar, MD
Gerald D. Suh, MD
Jason B. Surow, MD
Brian J. Szwarc, MD
Raj Tandon, MD
Michael B. Tom, MD
Joy L. Trimmer, JD (staff)
William Turner, MD
Keith M. Ulnick, DO
Richard W. Waguespack, MD
Michael D. Weiss, MD
Robert Weiss, MD
Samuel B. Welch, MD, PhD
Raymond Winicki, MD
Karen A. Wirtshafter, MD
Stanley Yankelowitz, MD
Irene Yu, MD
Todd A. Zachs, MD
John J. Zappia, MD
Warren H. Zelman, MD
Resident Capitol Club
Investment of $250+ Annually
Scott Chaiet, MD
Dollar-a-Day Club
Investment of 365+ Annually
Robert E. Adham, MD
Mehmet C. Agabigum, MD
Ravi P. Agarwal, MD
Michael Agostino, MD
J. Noble Anderson, Jr., MD
Lauren C. Anderson de Moreno, MD
Seilesh Babu, MD
David A. Bianchi, MD
David S. Boisoneau, MD
Dennis I. Bojrab, MD
William R. Bond, Jr., MD
K. Paul Boyev, MD
James T. Brawner, MD
Steven H. Buck, MD
Dennis Burachinsky, DO
Scott L. Busch, DO
Roy D. Carlson, MD
Ryan C. Case, MD
Ajay E. Chitkara, MD
James Z. Cinberg, MD
Anthony J. Cornetta, MD
Kent W. Cox, MD
Michael D’Anton, MD
John M. DelGaudio, MD
James C. Denneny III, MD
Robert W. Dolan, MD
John S. Donovan, MD
Jeffrey S. Driben, MD
David R. Edelstein, MD
Moshe Ephrat, MD
Michael D’Anton, MD
John M. DelGaudio, MD
James C. Denneny III, MD
Robert W. Dolan, MD
John S. Donovan, MD
Jeffrey S. Driben, MD
David R. Edelstein, MD
Moshe Ephrat, MD
Theodore W. Fetter, MD
Stephen M. Froman, MD
Michael J. Fucci, MD
Krishna M. Ganti, MD
Julie A. Goddard, MD
Frederick A. Godley III, MD
Debora W. Goebel, MD
Stephen A. Goldstein, MD
Steven I. Goldstein, MD
Ramez Habib, MD
Patrick Hall, MD
Ronald D. Hanson, MD
Stuart M. Hardy, MD
Brenda Hargett, CPA (staff)
Joseph E. Hart, MD, MS
James M. Hartman, MD
Sabine V. Hesse, MD
Arlis W. Hibbard, MD
Michael D’Anton, MD
John M. DelGaudio, MD
James C. Denneny III, MD
Robert W. Dolan, MD
John S. Donovan, MD
Jeffrey S. Driben, MD
David R. Edelstein, MD
Moshe Ephrat, MD
Michael D’Anton, MD
John M. DelGaudio, MD
James C. Denneny III, MD
Robert W. Dolan, MD
John S. Donovan, MD
Jeffrey S. Driben, MD
David R. Edelstein, MD
Moshe Ephrat, MD
Theodore W. Fetter, MD
Stephen M. Froman, MD
Michael J. Fucci, MD
Krishna M. Ganti, MD
Julie A. Goddard, MD
Frederick A. Godley III, MD
Debora W. Goebel, MD
Stephen A. Goldstein, MD
Steven I. Goldstein, MD
Ramez Habib, MD
Patrick Hall, MD
Ronald D. Hanson, MD
Stuart M. Hardy, MD
Brenda Hargett, CPA (staff)
Joseph E. Hart, MD, MS
James M. Hartman, MD
Sabine V. Hesse, MD
Arlis W. Hibbard, MD
John R. Houck, Jr., MD
John W. House, MD
Kenneth V. Hughes III, MD
Ofer Jacobowitz, MD, PhD
David M. Jakubowicz, MD
Robert E. Johnson, MD
Michael J. Kelleher, MD
Jeffrey H. Kerner, MD
Jay H. Klarsfeld, MD
Steven T. Kmucha, MD, JD
Michael J. Kortbus, MD
Kevin C. Krebsbach, MD
Greg Krempl, MD
Jeffery J. Kuhn, MD
Denis C. Lafreniere, MD
Pierre Lavertu, MD
David B. Lawrence, MD
Amy D. Lazar, MD
Joel F. Lehrer, MD
Jonathan A. Lesserson, MD
Sonya Malekzadeh, MD
Megan Marcinko, MPS (staff)
Jeffrey S. Masin, MD
Marc D. Maslov, MD
Phillip L. Massengill, MD
William A. McClelland, MD
Timothy M. McCulloch, MD
Valentin F. Mersol, MD
Abby C. Meyer, MD
Donna J. Millay, MD
David D. Morrissey, MD
Iman Naseri, MD
V. Rama Nathan, MD
Paul R. Neis, MD
James P. Oberman, MD
Douglas A. O’Brien, MD
J. David Osguthorpe, MD
Gregory S. Parsons, MD
Michael L. Patete, MD
Lisa Perry-Gilkes, MD
Kim E. Pershall, MD
Guy J. Petruzzelli, MD, MBA, PhD
Christopher P. Poje, MD
Eileen M. Raynor, MD
Michael J. Reilly, MD
John S. Rhee, MD, MPH
Grayson K. Rodgers, MD
Jeffrey D. Roffman, MD
Sarah L. Rohde, MD
Philip T. Rowan, MD
Phillip Rowan, MD
Greg S. Rowin, DO
Adam D. Rubin, MD
Hyman Ryback, MD
Daniel Santos, MD
John Scheibelhoffer, MD
Neil Schiff, MD
David N. Schwartz, MD
Rasesh P. Shah, MD
Frank G. Shechtman, MD
Katherine J. Shen, MD
Abraham I. Sinnreich, MD
Jonathan C. Smith, MD
Gary M. Snyder, MD
Christopher S. Song, MD
Neil M. Sperling, MD
Aaron T. Spingarn, MD
F. Thomas Sporck, MD
Robert J. Stachler, MD
James A. Stankiewicz, MD
Jayde M. Steckowych, MD
Jamie Stern, MD
Wendy B. Stern, MD
Michael G. Stewart, MD, MPH
Monica Tadros, MD
Thomas G. Takoudes, MD
Charles B. Tesar, MD
J. Regan Thomas, MD
Richard A. Tibbals, MD
Paulus D. Tsai, MD
Dale A. Tylor, MD
Eugenia M. Vining, MD
Hayes H. Wanamaker, MD
Jared M. Wasserman, MD
Daniel L. Wohl, MD
Danny Wong, MD
Arthur P. Wood, MD
Gayle E. Woodson, MD
Glen Y. Yoshida, MD
K. John Yun, MD
2013 General Member
David A. Abraham, MD
Allan L. Abramson, MD
Jason L. Acevedo, MD
Olubunmi A. Ajose-Popoola, MD
Mohammad M. Akbar, MD
Raymond Aldridge, MD
Keith J. Alexander, MD
Art A. Ambrosio, MD
Scott R. Anderson, MD
Larry L. Bailey, MD
John M. Barlow, MD
Christian H. Barnes, MD
Melynda A. Barnes, MD
James P. Bartels, MD
Richard Bauer, MD
Russell N. Beckhardt, MD
Mark G. Bell, MD
Thomas J. Benda, Sr., MD
Thomas J. Benda, Jr., MD
David F. Bennhoff, MD
Michael S. Benninger, MD
Michael P. Bernstein, MD
Shelley R. Berson, MD
Jay M. Bhatt, MD
Mahesh H. Bhaya, MD
Christopher M. Bingcang, MD
Mary Blome, MD
Jacob O. Boeckmann, MD
Peter C. Bondy, MD
I. David Bough, Jr., MD
Alexis C. Bouteneff, MD
Phyllis B. Bouvier, MD
Lawrence L. Braud, MD
Maury B. Bray III, MD
Michael J. Brenner, MD
Jean Brereton, MBA (staff)
Frank Allan Brettschneider, DO
Jenna W. Briddell, MD
David Brown, MD
Laura D. Brown, MD
Warren L. Buchalter, MD
Lawrence P. A. Burgess, MD
James E. Bush, MD
Richard K. Caldwell, MD
Rich Capparell (staff)
John M. Carter, MD
Margaret S. Carter, MD
Louis Chanin, DO
David R. Charnock, MD
Hamad Chaudhary, MD
Brian S. Chen, MD
Bradford S. Chervin, MD
Anthony E. Chin Loy, MD
Sukgi S. Choi, MD
Shawn C. Ciecko, MD
William B. Clark, MD
David S. Cohen, MD
Candice C. Colby, MD
Christian P. Conderman, MD
Bryant T. Conger, Jr., MD
Mary Pat Cornett (staff)
Carolyn A. Coughlan, MD
Thomas M. Crews, MD
Roger L. Crumley, MD, MBA
Lori L. Cudone, MD
Brian D. D’Anza, MD
Paul Davey, MD, PC
Nichole R. Dean, DO
Devang P. Desai, MD
Joseph R. Di Bartolomeo, MD
Karl W. Diehn, MD
Jayme R. Dowdall, MD
Thomas F. Dowling, MD
Norman S. Druck, MD
Carl Drucker, MD
Peter T. Dziegielewski, MD
Marc D. Eisen, MD, PhD
Dale C. Ekbom, MD
Michael S. Ellis, MD
B. Kelly Ence, MD
Jay B. Farrior, MD
Berrylin J. Ferguson, MD
Alberto T. Fernandez, MD
William I. Forbes III, MD, PhD
D. Scott Fortune, MD
Allen Foulad, MD
Mark L. Fox, MD
Paul C. Frake, MD
Marvin P. Fried, MD
Ellen M. Friedman, MD
Robert H. Furman, MD
Judith E. Gallagher, MD
Daniel Ganc, MD
John Paul Giliberto, MD
Aylon Y. Glaser, MD
Sharon H. Gnagi, MD
Lindsay I. Golden, MD
Rebecca D. Golgert, MD
Mariano E. Gonzalez-Diez, MD
Steven J. Green, MD
Nancy R. Griner, MD
Samuel P. Gubbels, MD
Yarah M. Haidar, MD
Marc David Hamburger, MD
Steven D. Handler, MD, MBE
Charles J. Harkins, MD
Michael S. Harris, MD
A. Kristina E. Hart, MD
Adrianna M. Hekiert, MD
Webb S. Hersperger, MD
Douglas M. Hildrew, MD
David L. Hilton, MD
Matthew L. Hinsley, MD
Ronald H. Hirokawa, MD
Barry Hirsch, MD
Brian Ho, MD
Paul T. Hoff, MD
Thomas C. Huang, MD
Robert J. Hughes, MD
Charles G. Hurbis, MD
Thomas M. Irwin Jr., MD
Jeffrey Jablon, MD
Neal Jackson, MD
Gary W. Jones, PhD
John W. Jones, MD
Stephanie L. Jones (staff)
Thomas C. Huang, MD
Robert J. Hughes, MD
Charles G. Hurbis, MD
Thomas M. Irwin Jr., MD
Jeffrey Jablon, MD
Neal Jackson, MD
Gary W. Jones, PhD
John W. Jones, MD
Stephanie L. Jones (staff)
D. Scott Fortune, MD
Allen Foulad, MD
Mark L. Fox, MD
Paul C. Frake, MD
Marvin P. Fried, MD
Ellen M. Friedman, MD
Robert H. Furman, MD
Judith E. Gallagher, MD
Daniel Ganc, MD
John Paul Giliberto, MD
Aylon Y. Glaser, MD
Sharon H. Gnagi, MD
Lindsay I. Golden, MD
Rebecca D. Golgert, MD
Mariano E. Gonzalez-Diez, MD
Steven J. Green, MD
Nancy R. Griner, MD
Samuel P. Gubbels, MD
Yarah M. Haidar, MD
Marc David Hamburger, MD
Steven D. Handler, MD, MBE
Charles J. Harkins, MD
Michael S. Harris, MD
A. Kristina E. Hart, MD
Adrianna M. Hekiert, MD
Webb S. Hersperger, MD
Douglas M. Hildrew, MD
David L. Hilton, MD
Matthew L. Hinsley, MD
Ronald H. Hirokawa, MD
Barry Hirsch, MD
Brian Ho, MD
Paul T. Hoff, MD
Thomas C. Huang, MD
Robert J. Hughes, MD
Charles G. Hurbis, MD
Thomas M. Irwin Jr., MD
Jeffrey Jablon, MD
Neal Jackson, MD
Gary W. Jones, PhD
John W. Jones, MD
Stephanie L. Jones (staff)
Russel Kahmke, MD
Lawrence Katin, MD
Scott L. Kay, MD
Kanwar S. Kelley, MD, JD
Paul E. Kelly, MD
Samuel C. Kerns, MD
Anita Konka, MD
Charles F. Koopmann, Jr., MD, MHSA
Todd A. Kupferman, MD
Steven L. Kutnick, MD
Michael J. Latshaw, MD
Dennis Lee, MD, MPH
Gregory T. Lesnik, MD
Thomas H. Lesnik, MD
Douglas Leventhal, MD
Katherine Lewis (staff)
Carl M. Lieberman, MD
Jennifer L. Lin, MD
Jeffrey C. Liu, MD
Brian C. Lobo, MD
Mark B. Logan, MD
Scott D. London, MD
Lily Love, MD
Rodney P. Lusk, MD
Frank A. Luzzi, MD
Bruce R. Maddern, MD
James R. Magnussen, MD
James A. Manning, MD
Frances E. Marchant, MD
Jonathan R. Mark, MD
Frank I. Marlowe, MD
Felipe J. Martinez, MD
Nicholas Mastros, MD
Bruce H. Matt, MD
Clement J. McDonald III, MD
Kathleen R. McDonald, MD
Bryan R. McRae, MD
Michael R. Menachof, MD
Albert L. Merati, MD
Ralph B. Metson, MD
Elias Michaelides, MD
Anya J. Miller, MD
Ron Mitzner, MD
Carl Moeller, MD
David F. Moore, Jr., MD
Willard B. Moran, Jr., MD
Michael D. Morelock, MD
Philip R. Morgan, MD
Jesse Moss Jr., MD
Kevin K. Motamedi, MD
James J. Murdocco, MD
James G. Murray, MD
John P. Neis, MD
Zephron G. Newmark, MD
Carrie L. Nieman, MD, MPH
Stephen Nogan, MD
David C. Norcross, MD
Raimundo L. Obregon, MD
John V. O’Neill, MD
Ryan K. Orosco, MD
Ralph G. Owen, Jr., MD
Othella T. Owens, MD
Stephen E. Parey, MD
Sanjay R. Parikh, MD
Mariah B. Pate, MD
Nilesh Patel, MD
Andrew D. Pedersen, MD
Ilya Perepelitsyn, MD
Jennifer Ann Pesola, DO
Linnea Peterson, MD
Luke Philippsen, MD
Brendan Pierce, MD
Timothy F. Pingree, MD
Colleen T. Plein, MD
Joel E. Portnoy, MD
William M. Portnoy, MD
William S. Postal, MD
William P. Potsic, MD
Robert B. Prehn, MD
Shannon P. Pryor, MD
Michael D. Puricelli, MD
Sanjeet Rangarajan, MD
Nikhila P. Raol, MD
David A. Reiersen, MD
Yvonne L. Richardson, MD
Anthony A. Rieder, MD
Brianne B. Roby, MD
Daniel Rocke, MD
Inell C. Rosario, MD
Eben L. Rosenthal, MD
Mark I. Rubinstein, MD
Ran Y. Rubinstein, MD
Marisa A. Ryan, MD
Stuart J. Sabol, MD
Ron Sallerson (staff)
Jordan Paul Sand, MD
Eric W. Sargent, MD
James E. Saunders, MD
Mary J. Scaduto, MD
Gordon F. Schaye, MD
George Schein II, MD
Michael Scherl, MD
Jonathan L. Schmidt, MD
Kristine Schulz, MPH
Jerome Steven Schwartz, MD
Curtis M. Seitz, MD
Merritt J. Seshul, MD
Michael Setzen, MD
David G. Sexton, MD
Priyanka Shah, MD
David Shamouelian, MD
Peter M. Shepard, MD
William M. Sheppard, MD
Michael J. Shinners, MD
Abraham Shulman, MD
Joseph D. Siefker, MD
John G. Simmons, MD
Michael J. Simmons, MD
Ameet Singh, MD
Lee P. Smith, MD
Ray Soletic, MD
Michael S. Srodes, MD
C. Richard Stasney, MD
Rebecca S. Stone, MD
George B. Stoneman, MD
Robert N. Strominger, MD
Mariel Stroschein, MD
Neelima Tammareddi, MD
Christopher G. Tang, MD
Rafael Tarnopolsky, MD
Thomas B. Thomason, MD
Prasad J. Thottam, DO
Tjoson Tjoa, MD
Jeremiah C. Tracy, MD
Debara L. Tucci, MD
John Martin Ulrich, DO
Emilio R. Valdes, Jr., MD
Zachary P. VandeGriend, MD
Peter M. Vila, MD
Valerie J. Vitale, MD
Angela Vong, MD
Matthew S. Voorman, MD
Mark A. Voss, MD
Kurtis A. Waters, MD
Mark K. Wax, MD
Roger E. Wehrs, MD
Debra G. Weinberger, MD
Adam S. Weisstuch, MD
Josh Werber, MD
Ralph F. Wetmore, MD
James A. White III, MD
Laura J. White, MD
Lauren C. White, MD
Peter F. White, MD
Chad Whited, MD
Neil P. Williams, MD
Kevin F. Wilson, MD
Meghan N. Wilson, MD
Peak Woo, MD
Kyle T. Yamamoto, MD
Eiji Yanagisawa, MD
C. Alan Yates, MD
Yuk Yee Yau, MD
Estelle S. Yoo, MD
William Gregory Young, Jr., MD
Lauren S. Zaretsky, MD
Alice S. Zhao, MD
Kevin L. Ziffra, MD
Michael Zoller, MD
2013 Group Practice Contributions
Advanced ENT & Allergy PLLC
Cape Fear Otolaryngology
Colden Seymour Ear, Nose, Throat & Allergy
For more information about ENT PAC and its applicable programs, visit www.entpac.org (log-in with your AAO-HNS user ID and password).
*Contributions to ENT PAC are not deductible as charitable contributions for federal income tax purposes. Contributions are voluntary, and all members of the AmericanAcademy of Otolaryngology-Head and Neck Surgery have the right to refuse to contribute without reprisal. Federal law prohibits ENT PAC from accepting contributions from foreign nationals. By law, if your contributions are made using a personal check or credit card, ENT PAC may use your contribution only to support candidates in federal elections. All corporate contributions to ENT PAC will be used for educational and administrative fees of ENT PAC, and other activities permissible under federal law. Federal law requires ENT PAC to use its best efforts to collect and report the name, mailing address, occupation, and the name of the employer of individuals whose contributions exceed $200 in a calendar year.