More from May 2014 - Vol. 33 No. 05

AAO-HNS Member Gregory W. Randolph, MD, FACE, who has worked closely with the AACE for many years presenting at their meetings and serving in leadership positions, has been dedicated to establishing otolaryngologist—head and neck surgeon eligibility for the FACE designation. He and fellow Academy supporters named here are pleased to extend the following information to you in concert with ACE and AACE colleagues.
The Fellow of the AmericanCollege of Endocrinology (FACE) designation is achievable by otolaryngologist-head and neck surgeons who provide a high standard of excellence, achievement, and quality of patient care given to their patients with endocrine disorders.
Physicians eligible to receive this honor must be members in good standing of the American Association of Clinical Endocrinologists (AACE) for at least three years. As such, otolaryngologist-head and neck surgeons seeking FACE distinction should apply for AACE membership if they meet certain criteria, such as 50 percent or more of their practice being dedicated to thyroid and parathyroid disorders. FACE recipients are honored with induction into the College at the ACE Convocation, which takes place during the AACE Annual Meeting. Fellows can then use the FACE post-nominal title to denote the honor.
AACE is eager to engage the otolaryngologist-head and neck surgeon community, which already has a great history of collaboration. In fact, Dr. Randolph has earned the FACE credential for his contribution to the management and treatment of thyroid cancer. He is also currently chair of the AACE Endocrine Surgery Committee and AHNS Endocrine Surgery Committee and a former AAO-HNSF International Coordinator and Endocrine Surgery Committee Chair. With this experience, he will welcome your interest. He has found that many AACE members focus on diseases of the thyroid and parathyroid glands and work well in partnership with head and neck surgeons.
AACE and ACE
Jeffrey I. Mechanick, MD, FACP, FACE, FACN, ECNU; president, AACE
Daniel Einhorn, MD, FACP, FACE; President, ACE
R. Mack Harrell, MD, FACP, FACE, ECNU; president-elect, AACE
Jeffrey R. Garber, MD, FACP, FACE; immediate past president, ACE
AAO-HNS/F
Richard W. Waguespack, MD; president
James L. Netterville, MD; immediate past president
AAO-HNS Endocrine Surgery Committee
Ralph P. Tufano, MD
Lisa A. Orloff, MD
David L. Steward, MD
Brendan C. Stack Jr., MD, FACE
David J. Terris, MD
Mark L. Urken, MD From the Drugs and Devices Committees
The development and use of the cochlear implant has been one the most significant advances in otolaryngology in the last century. It has truly revolutionized what we as otolaryngologists can offer to our patients with the most significant cases of hearing loss. While this “game-changing” medical device now stands in the limelight, its conception and early development was met with much resistance from recognized leaders in our field and great opposition from the deaf community, which considered it “genocide” to their culture.
The early work of Volta, Djourno, Eyries, and others eventually led William House to successfully implant a single electrode device into the cochlea of a human patient in 1961. Shortly thereafter, Blair Simmons and Robin Michelson placed multichannel implants. Subsequently, decades of dedication by surgeons, scientists, audiologists, and speech pathologists have enabled countless deaf children and adults to hear. Current implants allow recipients to gain sufficient open set speech to talk on a telephone, be mainstreamed to enter schools with hearing children, and use speech to function and communicate well in various professional and social settings. Studies have shown that many implant users perform at or near the level of normally hearing peers on certain speech testing batteries. The magnitude of these achievements is reflected in the awarding of the prestigious Lasker-DeBakey Clinical Medical Research Award to Graeme Clark, Ingeborg Hochmair, and Blake Wilson in 2013 for their efforts in the development of cochlear implants.
Despite these successes and numerous studies that have shown that cochlear implants are both clinically and cost effective, the overall utilization rate of this device in the United States is estimated at an astoundingly low 6 percent. Specifically for children in the U.S., the utilization rate is a much more favorable 50 percent of those who would qualify based on their audiological profile, largely due to the positive effects of the implementation of Universal Newborn Hearing Screening in 1999. Nevertheless, this still fails to compare to the 90 percent utilization rates in certain areas in Europe.
Several factors may be contributing to this low utilization rate. The first is that there is a low general awareness of cochlear implants and their potential benefits by both the public as well as primary care physicians. This poor understanding of candidacy and outcomes by referring providers may be a critical hurdle in getting the majority of patients who could benefit from an implant into the office of an otolaryngologist who can offer services. In addition, while there have been some positive changes from the early days of cochlear implantation, political resistance from organizations such as the deaf community, National Association of the Deaf, and the Autism Free America groups continue to exist.
Lastly, financial issues limiting hospitals and clinics continue to play a major role. With the metric of “quality of care” being on the forefront of healthcare governing bodies, hospital administrators, and the public, the development of widely accepted “best clinical practice” guidelines may provide a means to improve our ability to reach a greater proportion of the patients who could benefit from a cochlear implant. With the focused efforts of groups such as the recently incorporated American Cochlear Implant Alliance, we stand stronger to make progress on this front.
Despite these challenges, the number of patients receiving cochlear implants continues to grow and indications for surgery are further expanding. Initially a therapy offered only to adults with bilateral profound hearing loss, later it was approved for children two years and older in 1990 by the FDA. Today, children 12 months, and even younger in some cases, are gaining hearing with surgery. In addition to the lower limits of age, the increasing benefits of surgery outweighing the risks have permitted the audiological criteria for candidacy to evolve allowing for patients with less severe levels of hearing loss to qualify for implantation. While the standard adult candidate is someone who is considered to have little or no benefit from hearing aids based on speech recognition testing with scores of less than 50 percent on the ear to be implanted and less than 60 percent in the non-implanted ear or in the binaural condition, there has been much research demonstrating the benefits of cochlear implantation in patients with residual low frequency hearing. Hearing preservation techniques and hybrid implants providing electrical and acoustic stimulation have been used for years in Europe. These devices are currently in the final stages of approval by the Food and Drug Administration. This would provide individuals in the United States with high frequency sensorineural or “ski slope” hearing loss the opportunity to improve their communication function with a cochlear implant. In addition, currently there is much investigation in the areas of cochlear implantation for single-sided deafness and a therapy for tinnitus that may soon further expand the use of this innovative medical device.
Future technologies are aimed at enhancing sound quality, improving safety and reliability, and reducing costs. Incorporating technologies such as drug-eluting electrode arrays to reduce trauma from surgery, repairing damaged tissue biologically with stem cells, and developing new, more effective materials may provide avenues to bring the function of cochlear implants to the next level. With these ongoing efforts, we likely do not yet know the limits yet of this game-changing device. Rahul K. Shah, MD
George Washington University School of Medicine
Children’s National Medical Center, Washington, DC
Of course this is a rhetorical question—the modern patient safety and quality improvement, following the clarion call from the Institute of Medicine, is based on robust data, methodology, and outcomes. As such, it was an absolute surprise to many involved in PSQI (Patient Safety and Quality Improvement) research and initiatives that there was fraud and deceit amongst us.
I will try to summarize what is reported in the lay press about Dr. Charles Denham, MD, who at the time of a Justice Department settlement co-chaired a prominent committee, the NQF Safe Practices Committee, at the National Quality Forum. Please research this yourself to obtain the most accurate information.
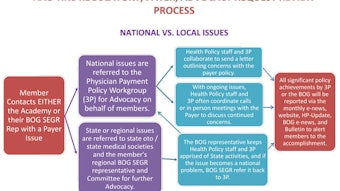
As members may recall, the Academy has physician and staff representation at the major quality organizations and associations, including (but not limited to) the Ambulatory Quality Alliance (AQA), National Quality Forum (NQF), AMA’s Physician Consortium for Performance Improvement (PCPI), and the Surgical Quality Alliance (SQA). It is a prescient decision for the Academy to be participating and involved in these organizations for more than a half-decade as we are well represented in the national landscape and able to adjust to changing influence. For example, if we were to plot the influence of these societies during the past many years, we would see evolving influence based on national priorities. Hence, the allegations of fraud of Dr. Denham hit close to home for our membership, as we are participants in the NQF.
The government alleges, while Dr. Denham co-chaired the NQF Safe Practices Committee, that a company he owned was provided contracts by CareFusion to promote its product, ChloraPrep. The product is used for surgical antisepsis, however the company was promoting its use off-label, which is not allowed. The allegation from the Justice Department was that the committee that Dr. Denham co-chaired was subjected to his influenced and that he personnally profited from payments from CareFusion. CareFusion was fined $40 million by the Justice Department. The story and the accompanying blog posts Wachter’s World are worth reading; indeed my co-chair of the AAO-HNS/F PSQI committee, David Roberson, MD, even opined on the post! My point being that this downfall, the first of such impact in the PSQI movement, has brought out many of our most respected safety experts to voice their sentiments.
I do not personally know Dr. Denham, but have heard him speak a few times. He is a gifted messenger and certainly a patient advocate. Nevertheless, the point of the column this month is to demonstrate that even a field as purely motivated as patient safety and quality improvement is susceptible to fraudulent behavior.
We must remain vigilant as Academy members and ensure that just because a group with good motives that is led by experts presents a claim or action does not a priori and without evidence make that claim substantiated. Academy member and journal editor, Richard M. Rosenfeld, MD, MPH, has done a tremendous job of asking the difficult questions about statistics, correlations, and causations when I have seen him at scientific meetings. This level of scrutiny is what we as individual Academy members can do with regards to statements from quality and safety organizations. We must not simply rollover and accept these mandates—the onus is on us as practicing providers to see the data and understand the rational for such measures. I have seen our membership in action and am confident that we always do push for the data and transparency.
In summary, the modern patient safety and quality improvement movement since the 2000s is not a fraud—the data is robust, medicine is embracing proven quality and scientific methodologies, and the outcomes of actual lives saved is exciting. However—caveat emptor: If a product sounds too good to be true, if an initiative has results that are not rational, and if someone seems conflicted—then double-check, as you may be right! If you can spare some time, these articles outlined below reinforce the absolute need for every organization engaging in these types of activities to have solid disclosure policies addressing of conflicts of interest.
References
http://online.wsj.com/article/BT-CO-20140109-709237.html, accessed March 9, 2014.
http://community.the-hospitalist.org/2014/01/30/patient-safetys-first-scandal-the-sad-case-of-chuck-denham-carefusion-and-the-nqf/, accessed March 9, 2014.
http://www.forbes.com/sites/michaelmillenson/2014/02/14/the-money-the-md-and-a-12-million-patient-safety-scandal/, accessed March 3, 2014.
Editor’s Note:
Please read Dr. Denham’s statement that can be found within the Wachter’s World article (http://community.the-hospitalist.org/2014/01/30/). Specifically it appears in the commentaries from a February 22, 2014, 7:41 pm reader.
We encourage members to write us with any topic of interest and we will try to research and discuss the issue. Members’ names are published only after they have been contacted directly by Academy staff and have given consent to the use of their names. Please email the Academy at qualityimprovement@entnet.org to engage us in a patient safety and quality discussion that is pertinent to your practice. A New Resource for AAO-HNS Members
Secondary data analysis can be an efficient research tool for identifying large numbers of cases for study without the time needed to collect primary data. For these reasons, there is increasing interest in secondary data analysis within the field of otolaryngology.
The AAO-HNSF Outcomes Research and Evidence-based Medicine (OREBM) Committee is pleased to announce that there is a new resource available to members on the AAO-HNS/F website. If you are conducting or looking to conduct research and are interested in using large datasets, there are many options available. But how do you decide which one is best for your purposes and your budget?
Under the guidance of Jennifer J. Shin, MD, SM, and Melissa A Pynnonen, MD, committee members and volunteers provide a list of existing datasets that may be appropriate for otolaryngology research. Each dataset is unique, with its own advantages, disadvantages, and nuances. To help newcomers identify a dataset that may be relevant for a particular research question, a basic overview of each dataset, example publications, and links for obtaining further information are provided. Some of the information presented includes: patient ages; practice setting, date range available; examples of publications; information about access; cost estimate(s); contact/website information; ease of use; and some pros/cons to using the data set for analysis. Datasets for inclusion were selected based on recommendations from members of the OREBM Committee.
Databases included on the site:
Kids’ Inpatient Database (KID)
MarketScan® Commercial Claims and Encounters and Medicare Supplemental and Coordination of Benefits
MarketScan® Health and Productivity Management/MarketScan® Health Risk Assessment
The National Ambulatory Medical Care Survey (NAMCS)
National Cancer Database (NCDB)
NationalHospital Ambulatory Medical Care Survey (NHAMCS)
Nationwide Emergency Department Sample (NEDS)
Nationwide Inpatient Sample (NIS)
SEER-Medicare
State Ambulatory Surgery Databases (SASD)
State Inpatient Databases (SID)
Surveillance, Epidemiology and End Results (SEER)
This list is not meant to be exhaustive, but rather a primer and foundation for members interested in beginning secondary data analysis in otolaryngology. The list will be reviewed periodically and updated as appropriate.
Special thanks to Emily F. Boss, MD, MPH; Amy Y. Chen, MD, MPH; Seth M. Cohen, MD, MPH; Dane J. Genther, MD; Eric J. Kezirian, MD, MPH; Frank R. Lin, MD; Gordon Sun, MD; and Bryan K. Ward, MD, for sharing their knowledge of these databases and assisting with this project.
We hope members find this to be a valuable resource and that it will help to facilitate new studies within the field of otolaryngology. To access the site, visit http://www.entnet.org/EducationAndResearch/Research-Databases.cfm.
If you have suggestions for additional databases or outcome instruments to be included on these sites or supplemental information that may be helpful, please let us know. Email Stephanie L. Jones, director of Research & Quality Improvement, at sljones@entnet.org.
Outcome Instruments
Did you know that the OREBM Committee also developed a web resource that presents key outcome instruments in otolaryngology-head and neck surgery? The site can assist the clinician looking to learn more about these tools and implement them in their practice or educate the more seasoned researcher who wants to stay up-to-date on the key tools and supporting literature. Learn more at http://www.entnet.org/EducationAndResearch/outcomesTools.cfm. Michael Setzen, MD
Immediate-Past Coordinator for Practice Affairs;
Manderly Cohen, MS CCC-SLP, and Jenna Minton, Esq., Senior Manager of Health Policy
For CY 2013, CMS finalized several key changes to reporting requirements associated with the provision of therapy services, and beginning on January 1, 2013, it implemented a claims-based data collection strategy to collect data on patient function. This policy encompassed a wide array of therapy services, including the Medicare Part B outpatient therapy benefit, therapy services under the Comprehensive Outpatient Rehabilitation Facility (CORF) benefit, and “incident to” services furnished by physicians or nonphysician practitioners, and included services furnished in hospitals, critical access hospitals (CAHs), skilled nursing facilities (SNFs), CORFs, rehabilitation agencies, home health agencies (when the beneficiary is not under a home health plan of care), and private offices.
CMS defines the term “therapists” as all practitioners who furnish outpatient therapy services, including physical therapists, occupational therapists, and speech-language pathologists in private practice and those therapists who furnish services in the institutional settings, physicians, and nonphysician practitioners (including physician assistants, nurse practitioners, and clinical nurse specialists, as applicable). Under this policy, claims for therapy services must now include non-payable G-codes and modifiers, which will allow the agency to capture data on the beneficiary’s functional limitations at various points during the provision of therapy. For therapy services being furnished that are not intended to treat a functional limitation, the therapist should use the G-code for “other” and the modifier representing zero.
A specific example of how this would apply in otolaryngology is when performing FEES/FEESST or providing therapy, including speech-language evaluation and treatment services for Medicare Part B beneficiaries, providers must report outcomes on claim forms. To facilitate this reporting, CMS established non-payable G-codes for reporting on claims for Medicare Part B beneficiaries receiving therapy services. Each non-payable G-code listed on the claim form must be accompanied with a severity/complexity modifier. The modifier represents the functional impairment on a 7-point severity/complexity scale.
G Codes
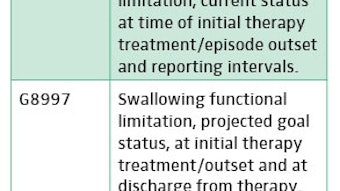
When billing FEES/FEESST CPT codes, specifically 92610 Evaluation of oral and pharyngeal swallowing function, 92612 Flexible fiberoptic endoscopic evaluation of swallowing by cine or video recording, and 92616 Flexible fiberoptic endoscopic evaluation of swallowing and laryngeal sensory testing by cine or video recording, where only an evaluation was performed and the patient will not be seen for therapy at the same facility, all three swallowing G-codes must be used when billing for the evaluation (G8996, G8997, and G8998) in addition to the appropriate severity modifier for each code.
Click here for a full list of available G-codes for reporting therapy services.
Severity Modifiers
Note: Corresponding National Outcomes Measurement System (NOMS) Functional Communication Measures [PDF] levels are listed here. Use of NOMS can assist with G-code and severity modifier selection, but is not required by CMS.
Members seeking additional information can access a full summary of this issue at http://www.entnet.org/Practice/CMS-News.cfm.