Alphabet Soup: Acronyms Advocates Need to Know
CBO: Congressional Budget Office. CBO produces independent analyses of budgetary and economic issues to support the Congressional budget process. CBO “scores” proposed bills to help lawmakers understand the cost or savings associated with a legislative package. CHHC: Congressional Hearing Health Caucus. CHHC is a bipartisan caucus of members from the U.S. House and Senate committed to supporting the U.S. needs of people with hearing loss and other auditory disorders. The AAO-HNS is a member of the Friends of the CHHC. CMS: Centers for Medicare & Medicaid Services. CMS is a federal agency within the U.S. Department of Health and Human Services. It is responsible for administering the Medicare program and working with states on administering their Medicaid programs. DHHA: Deaf and Hard of Hearing Alliance. DHHA is a coalition that seeks changes to federal public policy to help improve the quality of life for people who are deaf, hard of hearing, or have hearing loss. The AAO-HNS is a member of DHHA. HCLA: Health Coalition on Liability and Access. HCLA is a national advocacy coalition working to advance medical liability reform at the federal level. The AAO-HNS serves on the HCLA Board. HIT: Health Information Technology. Software and computer systems can now make medical records electronic, reducing paperwork and redundant forms. Federal and state governments are exploring numerous proposals to encourage the adoption of HIT while promoting quality initiatives and protecting patient privacy. IPAB: Independent Payment Advisory Board. The IPAB is an unelected government body established under the Patient Protection and Affordable Care Act. It is responsible for reducing the rate of growth in Medicare without affecting its coverage or quality. The Board is scheduled to implement its first proposal in 2015, although this is likely to be delayed. The AAO-HNS supports repeal of the IPAB. MedPAC: Medicare Payment Advisory Commission. MedPAC is an independent federal body established by the Balanced Budget Act of 1997. It is responsible for advising Congress on topics within the Medicare program, and more specifically, on issues dealing with payments to private health plans participating in Medicare and health providers that serve Medicare beneficiaries. MLR: Medical Liability Reform. MLR is a critical healthcare reform issue in the U.S. and a legislative priority for the AAO-HNS. Proponents of MLR are working to implement or amend legislation to lessen/cap excessive liability insurance costs for physicians while ensuring fair compensation for patients injured by negligent actions. PAC: Political Action Committee. PACs allow individuals with shared interests the opportunity to pool their voluntary donations to make contributions to federal candidates on behalf of the entire group. PACs represent a legal and ethical way to participate in the election process. ENT PAC (www.entpac.org) is the political action committee of the AAO-HNS. SGR: Sustainable Growth Rate. The SGR formula is a flawed expenditure target against which healthcare costs are compared. Generally, if annual healthcare costs fall below the target, Medicare reimbursement rates are increased. Conversely, if annual healthcare costs exceed the target, Medicare payment rates are decreased to reduce costs. Since healthcare costs tend to grow faster than the rate of inflation, the flawed formula has historically triggered annual Medicare physician payment cuts, which have typically been averted by Congressional action. The AAO-HNS supports repeal of the SGR formula. TIA: Truth in Advertising. The AAO-HNS and others in the physician community support state and federal efforts to implement TIA legislation requiring all healthcare providers to inform patients of their credentials and/or level of training in patient communications and marketing materials. Truth in advertising is an important component of providing patients with the best possible care. – See more at: http://aaobulletin.365.staging2.ascendmedia.com/Highlight.aspx?p=463&id=5937#sthash.44T2rmia.dpuf
CBO: Congressional Budget Office. CBO produces independent analyses of budgetary and economic issues to support the Congressional budget process. CBO “scores” proposed bills to help lawmakers understand the cost or savings associated with a legislative package.
CHHC: Congressional Hearing Health Caucus. CHHC is a bipartisan caucus of members from the U.S. House and Senate committed to supporting the U.S. needs of people with hearing loss and other auditory disorders. The AAO-HNS is a member of the Friends of the CHHC.
CMS: Centers for Medicare & Medicaid Services. CMS is a federal agency within the U.S. Department of Health and Human Services. It is responsible for administering the Medicare program and working with states on administering their Medicaid programs.
DHHA: Deaf and Hard of Hearing Alliance. DHHA is a coalition that seeks changes to federal public policy to help improve the quality of life for people who are deaf, hard of hearing, or have hearing loss. The AAO-HNS is a member of DHHA.
HCLA: Health Coalition on Liability and Access. HCLA is a national advocacy coalition working to advance medical liability reform at the federal level. The AAO-HNS serves on the HCLA Board.
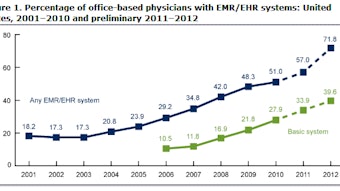
HIT: Health Information Technology. Software and computer systems can now make medical records electronic, reducing paperwork and redundant forms. Federal and state governments are exploring numerous proposals to encourage the adoption of HIT while promoting quality initiatives and protecting patient privacy.
IPAB: Independent Payment Advisory Board. The IPAB is an unelected government body established under the Patient Protection and Affordable Care Act. It is responsible for reducing the rate of growth in Medicare without affecting its coverage or quality. The Board is scheduled to implement its first proposal in 2015, although this is likely to be delayed. The AAO-HNS supports repeal of the IPAB.
MedPAC: Medicare Payment Advisory Commission. MedPAC is an independent federal body established by the Balanced Budget Act of 1997. It is responsible for advising Congress on topics within the Medicare program, and more specifically, on issues dealing with payments to private health plans participating in Medicare and health providers that serve Medicare beneficiaries.
MLR: Medical Liability Reform. MLR is a critical healthcare reform issue in the U.S. and a legislative priority for the AAO-HNS. Proponents of MLR are working to implement or amend legislation to lessen/cap excessive liability insurance costs for physicians while ensuring fair compensation for patients injured by negligent actions.
PAC: Political Action Committee. PACs allow individuals with shared interests the opportunity to pool their voluntary donations to make contributions to federal candidates on behalf of the entire group. PACs represent a legal and ethical way to participate in the election process. ENT PAC (www.entpac.org) is the political action committee of the AAO-HNS.
SGR: Sustainable Growth Rate. The SGR formula is a flawed expenditure target against which healthcare costs are compared. Generally, if annual healthcare costs fall below the target, Medicare reimbursement rates are increased. Conversely, if annual healthcare costs exceed the target, Medicare payment rates are decreased to reduce costs. Since healthcare costs tend to grow faster than the rate of inflation, the flawed formula has historically triggered annual Medicare physician payment cuts, which have typically been averted by Congressional action. The AAO-HNS supports repeal of the SGR formula.
TIA: Truth in Advertising. The AAO-HNS and others in the physician community support state and federal efforts to implement TIA legislation requiring all healthcare providers to inform patients of their credentials and/or level of training in patient communications and marketing materials. Truth in advertising is an important component of providing patients with the best possible care. – See more at: http://aaobulletin.365.staging2.ascendmedia.com/Highlight.aspx?p=463&id=5937#sthash.44T2rmia.dpuf