Clinical
Research
Professional Development
Practice Management
Advertise
Current Issue
Archives
Jobs/Events
About The Bulletin
July 2015 - Vol. 34 No. 06
Leading Edge
Registry, coding, and compassion
We continue to make progress on our “Road to a Registry.” This month’s Bulletin features an enlightening article about clinical registries, including the formation and benefits of Qualified Clinical Data Registries (QCDRs) and examples of successful registry operations.
Gripers and whiners
A recent “Piece of My Mind” essay by Scott I. Berman, MD, in the April 28 issue of JAMA talked about “gripers and whiners” in medicine. He made the point that “griping” is common across all professions and occupations: people complain about the difficulty of their work, yet continue in their jobs.
Vestibular Experiments in Space
Early in space exploration, research on the vestibular system was of great interest due to astronaut reports of spatial disorientation, nausea, and post-flight balance issues during the Apollo Program (1961-1972).1 This constellation of symptoms became known as Space Adaptation Syndrome (SAS).
No travel necessary to make an impact
Every August, Congress recesses for the entire month. The purpose of this “district work period” is for lawmakers to gather information and ideas for the remainder of the legislative session. This can include multiple public events with their constituents or more private meetings with local business leaders to discuss the effects of certain legislation.
FROM ACADEMY ADVANTAGE PARTNERThe most critical ICD-10 to-do’s
With political and practical realities solidifying October 1, 2015, as the national conversion to ICD-10, studies gauging how U.S. providers will fare appear somewhat mixed. A nationwide poll conducted earlier this year indicated that while most practices “pressed pause” in their readiness efforts last year, 81 percent expect to be ready on October 1. However, the study also found that only 21 percent of practices were “on track” and that nearly 20 percent hadn’t even started or were unaware of their preparations.
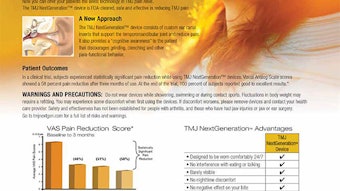
TMJ Next Generation
Supporting the future
The Centralized Otolaryngology Research Efforts (CORE) grants program plays a critical role in advancing the field of otolaryngology by providing support to research projects, research training, and career development.
Working together on performance measures
Measurement aligns with registry, payment models Quality metrics and performance measures have assumed center stage as payment progresses forward to alignment with quality of care and efficiency in care. To address Member needs for clinical quality measures, the AAO-HNSF launched the Performance Measures Task Force (PMTF) comprised of Richard M. Rosenfeld, MD, MPH, Chair, and Lisa E. Ishii, MD, MHS, James C. Denneny, MD, Richard V. Smith, MD, Jane T. Dillon, MD, MBA, Julie L. Goldman, MD, and David R. Nielsen, MD, in 2014. The Task Force held its first meeting in February 2015. Specific outcomes included a commitment to develop two prioritized sets of measures based on clinical practice guidelines (CPG), a continued collaboration with the AMA-convened Physician Consortium for Performance Improvement® (AMA-PCPI®) for measures testing, and exploration of tools that will facilitate faster development of measures from CPGs. Over the past year, the Foundation has produced a measures development strategy aligned with its registry initiative and new payment models to meet critical Member needs in the realm of quality reporting and support of Medicare and commercial reimbursement with an overarching goal of reinforcing the value of care provided by Members. The AAO-HNSF is moving forward for Members on three fronts in the realm of clinical quality measures. First, the Foundation took over ownership and stewardship of the AMA-PCPI® measures most applicable to our Members, which include acute otitis externa (AOE), adult sinusitis, and otitis media with effusion (OME) in December 2014. Each of the measures had time-limited endorsement from the government contractor for measure endorsement, the National Quality Forum (NQF). One of the key roles of measure owners and stewards is ensuring the continued validity and endorsement, as well as dissemination and use of the clinical quality measures in its portfolio. To this end, the acute otitis externa (AOE) and otitis media with effusion (OME) measure groups are under consideration in NQF for continued endorsement under their Head, Eyes, Ears, Nose, and Throat (HEENT) measures initiative. This particular NQF project seeks to identify and endorse clinical quality measures for accountability and quality improvement that address these structures. The NQF Committee overseeing this project has two Academy Member appointees, Kathleen Yaremchuk, MD, MSA, and Michael G. Stewart, MD, MPH. Dr. Rosenfeld will provide his expertise in responding to any questions from the panel during the AOE and OME measures review. Much work has been done behind the scenes to prepare the measures applications, identify all uses of the measures since their initial endorsement, gather all research on gaps in care these address, and all testing and reporting data for submission to NQF for review. During May and June conference calls were held with the NQF HEENT Committee overseeing this initiative. The process concluded with a formal presentation of the measures by the AAO-HNSF to NQF in June. As the AOE and OME measures were prepared for NQF endorsement, the Foundation launched its own review of the adult sinusitis measures. This review of the measure specifications highlighted several issues that may have impacted Members’ quality reporting in 2014. Staff worked closely with the Centers for Medicare & Medicaid Services (CMS) executive leadership and with the Physician Quality Reporting System (PQRS) vendors to assure correct reporting for Academy Members in 2014 and 2015. Complete revisions to these measures will be in place for 2016 reporting as well. These measures are now under Academy ownership and stewardship, which will allow for continued utilization in the PQRS program and for broad dissemination to assure use. The Foundation’s work on the second front in clinical quality measures centers on its work to assure that an adequate pipeline of measures is available for Maintenance of Certification (MOC) by otolaryngologists and other physicians for quality improvement and quality reporting purposes. This is where the registry will play a critical role. With a registry, the Foundation will be able to utilize EHR data as well as claims data to craft quality metrics quickly for inclusion in quality reporting programs such as PQRS, Meaningful Use, and the Value-Based Modifier. Concurrently, it is also critically important that the AAO-HNSF disseminate its current measures as broadly as possible to improve patient care and outcomes. To this end, the Foundation has secured inclusion in PQRS of the adult sinusitis and acute otitis externa measures and measure groups. Academy staff has also researched every measure available in PQRS that might have applicability to Member practices and has organized all of these measures and related information on the AAO-HNS/F website at www.entnet.org/content/quality-measures. The third domain of measure activity focuses on staying abreast of changes to federal rules and regulations in the realm of quality reporting. At this point, it is worthwhile to share just what is happening with your Foundation measures for quality reporting in 2015. This is where measures have a profound impact for Members. As we noted earlier, AOE and sinusitis measures are contained within PQRS. This year, both Meaningful Use and the Value Based Modifier will be linked to PQRS. Concurrently, this is the year when fines will be levied for failure to report in PQRS with downstream ramifications into other quality reporting programs—all of which could have an impact on reimbursement in 2017. The most important point is to start early. To avoid penalties and fines, report to PQRS in 2015. Do you report to PQRS as an individual or as a group? You may report through the PQRSwizard® made available through the Academy, an EHR, or a registry. You may report either as an individual or as a group. This is an important decision to make early. Reporting as an individual If you decide to report individually, you may report using measure groups. If you choose this option, you must report on one measures group on a 20-patient sample, a majority of which (at least 11 out of 20) must be Medicare Part B patients. If you choose to create your own list of measures from the table below, you will have to select nine measures covering three quality domains and report for at least 50 percent of your Medicare Part B patients. Reporting as a group If you choose to report as a group, you must first register with CMS. Then, you will identify nine measures from the individual measures list below that cross at least three quality domains. You will report for at least 50 percent of your group’s Medicare Part B patient population. For more information on group reporting, visit www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Registry-Reporting.html. The good news is the Academy has made the process of measure selection easier by having identified all the measures that could be used by Academy Members and sorted them by quality domain for ease of use. The measures highlighted in red were developed and stewarded by the Academy. To secure information on all of the individual measures contained in the table at right, visit www.entnet.org/content/individual-quality-measures. It is clear with the passage of H.R. 2 Medicare Access and CHIP Reauthorization Act of 2015, the need for quality measures will continue well into the future. The Academy recognizes the complexity and difficulty of the CMS quality reporting and hence, the decision to invest resources into quality measurement development specific to our specialty. 2015 National Quality Strategy Domains (Individual/Claims Measures) Patient Safety Person and Caregiver- Centered Experiences and Outcomes [Patient and Family Engagement] Communication and Care Coordination Effective Clinical Care [Clinical Processes/Effectiveness] Community/ Population Health [Population/Public Health] Efficiency and Cost Reduction [Efficient Use of Healthcare Resources] Perioperative Care: Selection of Prophylactic Antibiotic – First OR Second Generation Cephalosporin PQRS #21 Patient Centered Surgical Risk Assessment and Communication PQRS #358 Medication Reconciliation PQRS #46 Controlling High Blood Pressure PQRS #236 Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention PQRS #226 Acute Otitis Externa (AOE): Systemic Antimicrobial Therapy – Avoidance of Inappropriate Use PQRS #93 Perioperative Care: Discontinuation of Prophylactic Parenteral Antibiotics (Non- Cardiac Procedures) PQRS #22 Optimal Asthma Control PQRS #398 Care Plan PQRS# 47 Acute Otitis Externa (AOE): Topical Therapy PQRS #91 Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented PQRS #317 Adult Sinusitis: Antibiotic Prescribed for Acute Sinusitis (Appropriate Use) PQRS #331 Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in All Patients) PQRS #23 Functional Outcome Assessment PQRS #182 Diabetes: Hemoglobin A1c Poor Control PQRS #1 Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan PQRS #128 Adult Sinusitis: Appropriate Choice of Antibiotic: Amoxicillin Prescribed for Patients w/ Acute Bacterial Sinusitis PQRS #332 Perioperative Temperature Management PQRS #193 Falls: Plan of Care PQRS #155 Asthma: Pharmacologic Therapy for Persistent Asthma Ambulatory Care Setting PQRS #53 Preventive Care and Screening: Influenza Immunization PQRS #110 Adult Sinusitis: CT for Acute Sinusitis (Overuse) PQRS #333 Falls: Risk Assessment PQRS #154 Functional Deficit: Change in Risk-Adjusted Functional Status for Patients with Neck, Cranium, Mandible, Thoracic, Spine, Ribs, or Other General Orthopedic Impairments PQRS #223 Immunizations for Adolescents PQRS #394 Adult Sinusitis: More than One CT Scan Within 90 Days for Chronic Sinusitis (Overuse) PQRS #334 Documentation of Current Medications in the Medical Record PQRS #130 Biopsy Follow-Up PQRS #265 Tobacco Use and Help with Quitting Among Adolescents PQRS #402 Appropriate Treatment for Children w/Upper Respiratory Infection PQRS #65 Radiology Exposure Time Reported for Procedures Using Fluoroscopy PQRS #145 Pain Assessment and Follow-Up PQRS #131 Appropriate Testing for Children with Pharyngitis PQRS #66 Pneumonia Vaccination Status for Older Adults PQRS #111 Reporting as individuals For physicians reporting as individuals, you may use these clinical quality measures groups or the other measures groups listed on our web site at www.entnet.org/content/quality-measures-groups. Sinusitis Measures Group Measure #130 Documentation of Current Medications in the Medical Record Measure #131 Pain Assessment and Follow-Up Measure #226 Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention Measure #331 Adult Sinusitis: Antibiotic Prescribed for Acute Sinusitis (Appropriate Use) Measure #332 Adult Sinusitis: Appropriate Choice of Antibiotic: Amoxicillin Prescribed for Patients with Acute Bacterial Sinusitis (Appropriate Use) Measure #333 Adult Sinusitis: Computerized Tomography (CT) for Acute Sinusitis (Overuse) Acute Otitis Externa Measures Group Measure #91 Acute Otitis Externa (AOE): Topical Therapy Measure #93 Acute Otitis Externa (AOE): Systemic Antimicrobial Therapy – Avoidance of Inappropriate Use Measure #130 Documentation of Current Medications in the Medical Record Measure #131 Pain Assessment and Follow-Up Measure #154 Falls: Risk Assessment Measure #155 Falls: Plan of Care Measure #226 Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention Measure #317 Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented
Registry 101
Patient registries are organized systems for patient data collection. Often developed and maintained by specialty societies, they can serve a number of purposes, with data collected for scientific, policy, or clinical reasons.
Research and quality
The Foundation’s 2015/2016 strategic plan outlines several major initiatives that reside in the Research and Quality (R & Q) business unit. It is an exciting time for R & Q, as these interrelated initiatives will provide valuable new quality tools for our Members.
EUGENE N. MYERS, MD INTERNATIONAL LECTURE ON HEAD AND NECK CANCER“Care and Rehabilitation of Patients Treated for Advanced Laryngeal Cancer”
After earning his medical degree in 1972 at the University of Utrecht, Dr. Hilgers completed his residency at the University of Amsterdam and his head and neck fellowship at the Netherlands Cancer Institute in 1978.
HOWARD P. HOUSE, MD MEMORIAL LECTURE FOR ADVANCES IN OTOLOGY“Modern Otology: A Nexus of Surgery, Neuroscience, and Biotechnology”
Scientists have known for 60 years that there is a battery-like power in the inner ear of mammals. But it took a team led by Konstantina Stankovic, MD, PhD, and scientists from MIT to figure out how to access that battery and begin assessing its potential.
JOHN CONLEY, MD, LECTURE ON MEDICAL ETHICS “What Makes a Great Surgeon?”
G. Scott Morris, MD, is a physician (board certified family practice), an ordained United Methodist minister (St. John’s United Methodist Church in Memphis), and the founder of a clinic (Church Health Center) that serves 65,000 people with primarily volunteer physicians and other healthcare providers.
H. BRYAN NEEL III MD, PHD DISTINGUISHED RESEARCH LECTURE“Leading the Biomedical Revolution in Precision Health: How Stanford Medicine Is Developing the Next Generation of Health Care”
The H. Bryan Neel III MD, PhD, Distinguished Research Lecture, funded by the Neel family and friends, was established to disseminate information on new developments in biomedical science to the otolaryngologic community. Lecturer: Lloyd B. Minor, MD Lloyd B. Minor, MD, scientist, surgeon, and academic leader, may be best known for identifying and coming up with a surgical correction for a disabling ear disorder called “superior canal dehiscence syndrome.” He is the Carl and Elizabeth Naumann Dean of the Stanford University School of Medicine, a position he has held since December 1, 2012. He is also a professor of otolaryngology–head and neck surgery and a professor of bioengineering and of neurobiology, by courtesy, at Stanford University. As Dean, Dr. Minor is leading the Campaign for Stanford Medicine, which seeks to sponsor innovation, transform patient care, and empower future leaders at the school. Beyond that, he challenges the U.S. healthcare system for comprehensive reforms to correct two systemic problems: very high costs, but not commensurate great results. He says it will require a team approach to both lower the cost of care and improve outcomes. He predicts technology will be a major part of the correction. Dr. Minor earned his bachelor’s and medical degrees from Brown University, and trained at Duke University and the University of Chicago medical centers. Before moving to Stanford, he was provost in The Johns Hopkins University School of Medicine. He has been honored for his research, and in 2012, was elected to the prestigious Institute of Medicine of the National Academy of Sciences.
COTTON-FITTON ENDOWED LECTURE IN PEDIATRIC OTOLARYNGOLOGY“Pediatric Otolaryngology: The Value Proposition of Subspecialty Training”
Marci Lesperance, MD, is professor of otolaryngology-head and neck surgery and division chief of pediatric otolaryngology at the University of Michigan Health System. She has a passion for otolaryngology and for seeing research advances translated into patient care.
Mission brings cleft lip/palate procedures to PeruExpanded from the print edition
What a whirlwind of a mission trip we had in Peru! Over the course of a week, 28 team members volunteering from the Pacific Northwest of the United States traveled to the Pacific Northwest of Peru.
The Academy needs you! Fill out a RUC survey
The Academy needs experts three times a year to fill out RUC surveys for the AMA Specialty Society/Relative Value Update Committee.
WIO: role models, trail blazers
Take advantage of the extraordinary networking and mentoring opportunities at this year’s WIO activities at the Annual Meeting. Learn about the incredible activities and career trajectories of some of our most respected leaders and interact in person.
2015 AAO-HNS/F Leadership Forum—a resident’s perspectiveExpanded from the print edition
Author and scholar on leadership Warren Bennis said, “Leadership is the capacity to translate vision into reality.” This was the take-away point I got from the annual AAO-HNS/F Leadership Forum in Arlington, VA, held March 14-16, 2015.
One humanitarian mission: two perspectives Expanded from the print edition
Since 2009, several otolaryngology-head and neck surgery trips have been organized to Eldoret, Kenya. The trips are part of an overarching program, the Indiana University-Kenya AMPATH Partnership (ampathkenya.org). Months of planning in both the United States and Kenya culminate in an intense two-week “ENT Camp,” which provides medical and surgical care, training, and relationship building between the U.S. and Kenyan otolaryngologists.
The expansion of fellowship training and the modern-day residentExpanded from the print edition
In 1994, Byron Bailey, MD, and Robert H. Miller, MD, MBS, examined the explosion in the amount of otolaryngology subspecialty programs and number of fellowship trainees.1,2 By 1994, 25 percent of the 260 otolaryngology residents were entering fellowship.2
BOARD OF GOVERNORSHow to be a more effective medical board memberExpanded from the print edition
When doctors get together they complain, a lot. This could be a good description of most hospital medical boards, even yours. However, better hospitals have built a different doctor relationship, which makes the medical board an instrument of change, a launching pad for new programs, and a forum for constructive dialogue.
2015 AAO-HNS Election results
The AAO-HNS extends its greatest appreciation to the candidates of the 2015 Election for their dedication and willingness to serve. The Nominating Committee presented the membership with an outstanding slate of candidates.
State Trackers, take a bow
With most state legislatures adjourned for the year, the AAO-HNS sincerely thanks its State Trackers who helped make 2015 another successful year. Despite their full workloads and family obligations, these physician leaders took action and volunteered their time to closely monitor and report on legislative activity in their statehouses.
As Meaningful Use changes, we’re advocating for you
As Members know, the Health Policy team has actively worked not only to educate Members on the Centers for Medicare & Medicaid’s (CMS) Electronic Health Records (EHR) Meaningful Use (MU) Incentive Program, but also to advocate on behalf of Members so that your needs and experiences are best represented within the program.