Changing Lives in Rwanda, the Land of a Thousand Hills
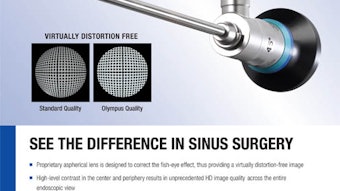
Yi-Hsuan E. Wu, MD Tufts Medical Center Boston, MA Inspiring. Refreshed. Energizing. Humbled. Those are some of the words my fellow team members and I use when describing our mission experience. With the help of a grant from the AAO-HNSF Humanitarian Efforts Committee, I had the privilege of joining Medical Missions for Children (MMFC) on its annual trip to Gitwe, Rwanda, in March to treat patients with endemic goiter due to iodine deficiency. Jagdish K. Dhingra, MD, has led the team, made up of 15 healthcare professionals and volunteers from the United States and Rwanda, for the past seven years. We arrived with 44 pieces of luggage in tow, including instruments, electrosurgical generators, and medications. The first day was spent turning two nearly empty rooms of the hospital into a functional operating room and recovery unit. With the help of Vianney Ruhumuliza, our in-country partner, prescreened patients were already at the hospital awaiting our evaluation and hopefully, surgical intervention. One woman had walked for three days for her chance to meet us. Unfortunately, not everyone with an operable goiter was able to be treated during our short time in Gitwe. These patients were given follow-up instructions and asked to return next year. Throughout the week, we took note to be thankful for the amenities taken for granted back home. Power went out unpredictably and frequently during surgeries, often leaving the surgeons without the ability to use electrocautery and the anesthesiologists with the task of keeping patients ventilated with an Ambu bag. Without a sterile processing unit (only a small autoclave), the surgical technologists diligently cleaned and packed the instruments between operations and rationed the use of clean towels, drapes, and sponges. Despite these hurdles, the team completed 25 subtotal thyroidectomies in six days. Everyone will remember Liliane, a friendly and attractive young woman with a contagious smile and an enormous goiter that involved her entire neck and extended to her left ear. Her surgery was the longest and most challenging. It was particularly rainy that day, and we lost power a few times during her seven-hour procedure to remove the two-pound mass from her neck. She had lost a fair amount of blood and also required nasogastric tube feeds for a few days. The team celebrated each step in her recovery, from drain and staple removals to finally being able to tolerate a regular diet. Despite being away from her children for nearly two weeks while recuperating in the hospital, Liliane smiled every day. Our last day in Gitwe was filled with hugs and “murakoze” (“thank you” in Kinyarwanda). In return, we are thankful for the opportunity to change lives and to “return to the essence of the profession,” as well expressed by David Gregg, MD, one of the attending surgeons on the team. I remain touched by every patient’s gratitude and positive attitudes and look forward to my next medical mission trip.
 Meeting a patient during morning rounds.
Meeting a patient during morning rounds.Yi-Hsuan E. Wu, MD
Tufts Medical Center
Boston, MA
Inspiring. Refreshed. Energizing. Humbled.
Those are some of the words my fellow team members and I use when describing our mission experience. With the help of a grant from the AAO-HNSF Humanitarian Efforts Committee, I had the privilege of joining Medical Missions for Children (MMFC) on its annual trip to Gitwe, Rwanda, in March to treat patients with endemic goiter due to iodine deficiency. Jagdish K. Dhingra, MD, has led the team, made up of 15 healthcare professionals and volunteers from the United States and Rwanda, for the past seven years.
We arrived with 44 pieces of luggage in tow, including instruments, electrosurgical generators, and medications. The first day was spent turning two nearly empty rooms of the hospital into a functional operating room and recovery unit. With the help of Vianney Ruhumuliza, our in-country partner, prescreened patients were already at the hospital awaiting our evaluation and hopefully, surgical intervention. One woman had walked for three days for her chance to meet us. Unfortunately, not everyone with an operable goiter was able to be treated during our short time in Gitwe. These patients were given follow-up instructions and asked to return next year.
 Lilane before and after her thyroid lobectomy.
Lilane before and after her thyroid lobectomy.Throughout the week, we took note to be thankful for the amenities taken for granted back home. Power went out unpredictably and frequently during surgeries, often leaving the surgeons without the ability to use electrocautery and the anesthesiologists with the task of keeping patients ventilated with an Ambu bag. Without a sterile processing unit (only a small autoclave), the surgical technologists diligently cleaned and packed the instruments between operations and rationed the use of clean towels, drapes, and sponges.
Despite these hurdles, the team completed 25 subtotal thyroidectomies in six days. Everyone will remember Liliane, a friendly and attractive young woman with a contagious smile and an enormous goiter that involved her entire neck and extended to her left ear. Her surgery was the longest and most challenging. It was particularly rainy that day, and we lost power a few times during her seven-hour procedure to remove the two-pound mass from her neck. She had lost a fair amount of blood and also required nasogastric tube feeds for a few days. The team celebrated each step in her recovery, from drain and staple removals to finally being able to tolerate a regular diet. Despite being away from her children for nearly two weeks while recuperating in the hospital, Liliane smiled every day.
Our last day in Gitwe was filled with hugs and “murakoze” (“thank you” in Kinyarwanda). In return, we are thankful for the opportunity to change lives and to “return to the essence of the profession,” as well expressed by David Gregg, MD, one of the attending surgeons on the team.
I remain touched by every patient’s gratitude and positive attitudes and look forward to my next medical mission trip.