Spring forward
As we transition into the spring of 2015 the AAO-HNS is in the process of unveiling a number of changes that we hope will be of value to our Members.
By James C. Denneny III, MD, AAO-HNS/F EVP/CEO

The AAO-HNS hosted a March 13th “Otolaryngology Strategic Summit” attended by representatives of 16 Societies including the American Academy of Facial Plastic and Reconstructive Surgery (AAFPRS), American Academy of Otolaryngic Allergy (AAOA), American Academy of Otolaryngology—Head and Neck Surgery (AAO-HNS), American Broncho-Esophagological Association (ABEA), American Board of Otolaryngology (ABOto), American College of Surgeons, American Head and Neck Society (AHNS), American Laryngological Association (ALA), American Neurotology Society (ANS), American Otological Society (AOS), Otolaryngology Program Directors Organization (OPDO), American Rhinologic Society (ARS), American Society of Geriatric Otolaryngology (ASGO), American Society of Pediatric Otolaryngology (ASPO), Society of University Otolaryngologists–Head and Neck Surgeons (SUO), and The Triological Society (TRIO).
Collegiality was high and discussions were stimulating throughout the day. The overall themes of the meeting were communication, integration, and dissemination, and the mechanisms to accomplish these.
Several areas of collaboration were discussed including exploring an integration of specialty society committees with those of the AAO-HNS, developing and maintaining a list of specialty society committee representatives and preferred lines of communications for each specialty, working toward a true “Annual Otolaryngology Meeting,” and defining expectations and roles for all organizations that complement and reinforce each other.
The Specialty Society Advisory Committee (SSAC), chaired by Richard M. Rosenfeld, MD, MPH, representing ASPO, will hold a meeting at COSM. Discussions will center around the role and value that this advisory group to the AAO-HNS Boards of Directors should assume as well as ways to increase the group’s effectiveness. There was acknowledgement that there will be degrees of interaction among the family of specialty groups.
Post event surveys indicated that the overall satisfaction of the meeting was 4.3 (1 being “poor” and 5 being “excellent”) and the value to the specialty was 4.6. There was enthusiasm for continued dialogue and regular events to keep communications open. I want to personally thank all who attended this meeting representing their respective organizations.
This year the AAO-HNS will move to a spring election to be held in May. The Election Review Task Force, chaired by Richard W. Waguespack, MD, recommended moving the elections to May to closely follow the Candidate’s Forum at the BOG meeting in March. Ideally this schedule will increase voter participation and interest in our elective process. The successful candidates will be oriented and integrated into their respective positions prior to the Annual Meeting so they can be prepared to contribute immediately. Guidelines for the elections were reviewed and campaigning activities more clearly defined. At this year’s Candidates Forum Gregory W. Randolph, MD, and Mark K. Wax, MD, were presented as the outstanding president-elect candidates for 2015.
Our annual meeting coordinators, Sugki S. Choi, MD, and Eben L. Rosenthal, MD, have unveiled a plan that will expand the learning opportunities in a more flexible co-mingled schedule at our meeting in Dallas. The Foundation will now offer Instruction Courses throughout the day as well as extension of other didactic programming into afternoon timeslots. This should allow our attendees an opportunity to tailor and organize their experience to meet their needs. Educational and social opportunities for our international attendees are also being expanded and stratified in a fashion that can maximize their meeting experience. Drs. Choi and Rosenthal have demonstrated exceptional leadership in moving forward these annual meeting enhancements. They will also be leading the transition from our current dual coordinator role (Coordinators for Scientific Program and Instruction Courses) to a single “Coordinator for Meetings.”
The obvious need and benefit of having a unified up-to-date curriculum for otolaryngology has been recognized for some time. Sonya Malekzadeh, MD, will be leading the AAO-HNSF MOC/Curricula Task Force to evaluate the feasibility of producing this valuable roadmap for both primary and continuing educational programs. Multiple stakeholders will be represented on this task force including the specialty societies, the ABOto, AADO, OPDO, and SUO. This massive project will benefit not only current trainees but also practicing otolaryngologists as they pursue MOC requirements.
We have experienced significant growth in the amount of international participation at our meetings and with our educational products. We have continued to try to enhance and improve the experience for international attendees. Conversations with our past Coordinators for International Affairs as well as prominent international otolaryngologists have helped shape our offerings to international participants. Our president, Gayle E. Woodson, MD, is in the process of selecting a task force to review all aspects of our international program. We value the participation and contributions of our international colleagues and continue to look for ways to improve their experience. James E. Saunders, MD, our current Coordinator for International Affairs, has been very active in the humanitarian community as well as helping us gather information on preferences from our international colleagues.
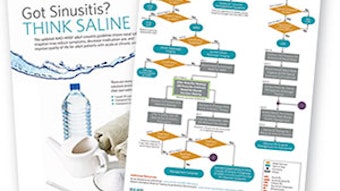
The AAO-HNSF has just released the updated version of our Clinical Practice Guidelines (CPG) on Adult Sinusitis this month. CPG’s require a regular update and maintenance process to ensure validity and appropriateness to patient care. This is a very work intensive process and we thank Richard M. Rosenfeld, MD, MPH, and Jay F. Piccarillo, MD, the chair and co-chair of the workgroup that produced this update. I would also like to thank all of our volunteers at work on the clinical practice guidelines as well as the quality measures that are crucial for our Members as we move forward into quality-based payment reform.