More from June 2014 - Vol. 33 No. 06

Given the uncertainty of today’s healthcare environment, what do you perceive as challenges and possible solutions to implementing the Academy’s strategic plan?
Paul M. Imber, DO
Is it kismet that I write my response to this provocative question on the evening that the Senate passes the 17th band-aid to the SGR debacle in 11 years, in spite of the potential to pass a bicameral, bipartisan permanent fix to the problem? The legislation also will delay ICD-10 implementation
by 12 months, and redirect savings from “misvalued codes” to “undervalued codes” and capture any excess as budget savings.
Advocacy is the ultimate tool of the Academy, as our members strengthen our presence with state and federal legislators. We can connect with our policy makers through the I-GO Program and obtain information from the biweekly Legislative Advocacy Network. Our Government Affairs staff members are superb stewards of our legislative interests, and are available resources to the membership to enhance engagement and unity.
The ever-changing reimbursement environment is replete with new, innovative experiments. The Academy can function as a research clearinghouse, collaborating the different structures and data from these projects, and sharing this information with the members to preclude repetition of failures and promote the proliferation of successes. The 3P is already in place to facilitate this process.
The need for practice and quality performance will be a component of any forthcoming payment reform program. The Academy needs to further sponsor the development of clinical guidelines, based on evidence-based research. The membership needs to avail itself of this knowledge.
The strategic plan can adapt in its direction, while maintaining its precepts, with appropriate leadership and counsel.
Jay S. Youngerman, MD
Challenges:
Ever increasing demands on physicians from patients, government, insurers, and businesses are driving the uncertainty in today’s healthcare environment.
First, the goal of higher quality and more efficient care is shared by all, but resulting regulations and metrics have encouraged standardization and bureaucracy at the expense of the best personalized care.
Second, as our colleagues become employees of large hospitals or groups, the shift of both daily and long-term decision-making from physician to administrator has diminished our collective influence on the way we practice.
Finally, information technology, in the form of cumbersome electronic records and online clinician ratings and patient information, has put us on the defensive rather than on the forefront.
Solutions:
Education: The Academy must be the recognized source on the web for the education of both clinicians and patients. Meetings must remain an indispensable forum for discourse, networking, and camaraderie.
Research and quality: Through evidence we can steer the tide of performance and efficiency toward truly better care for our patients. We must support models that simultaneously promote quality, reduce waste, and protect reimbursement.
Advocacy: Only the Academy can represent the specific interests of otolaryngology. We must continue to represent our specialty relentlessly at the national, state, and local levels.
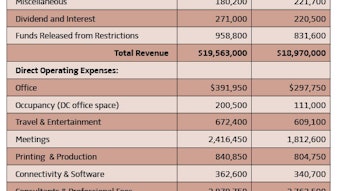
Sustainability: We must make particular efforts to attract our residents and young physicians, as well as the administrators, subspecialists, and physician extenders who are critical to our field. As the former Chair of the Board of Governors Development Committee, I will continue to encourage philanthropy through the Millennium Society, Women in Otolaryngology, and endowments. We must also encourage new revenue streams, corporate support, NIH grants, and CORE grant sponsors. The budget has been prepared on a cash basis. This basis is important to reflect the ability for an organization to meet its true financial obligations, regardless of whether the cash outlay is a true “expense” or merely balance sheet accounting. The FY15 budget prioritizes the direction of the BODs and is based on conservative estimates of both revenues and expenses. The FY15 balanced budget is presented at $18.97M, about three percent lower than the FY14 budget of $19.56M.
Nearly 75 percent of FY15 revenue, $14.06M, is budgeted to come from two major areas: membership dues and Annual Meeting revenue. Membership dues include a calendar year 2015 dues increase. Annual Meeting registration revenue is budgeted slightly higher than Vancouver but this is offset by a reduction in Instruction Course fees, mainly due to the change in the Annual Meeting length. Budgeted revenue reductions are in royalties income, which is primarily due to a change in presentation of Bulletin royalties, which are now reflected net of expenses, and corporate and individual support, which reflects the expected continued decline of unrestricted giving. As presented, overall revenues are down as compared to FY14; however, an ongoing commitment has been made to focus on increasing revenues as a result of new products and services.
To balance the budget with the expected reduction in revenue sources, operating expenses had to be thoroughly reviewed, streamlined, and affirmed as related to the strategic plan. The expenses for the AAO-HNS/F are separated into two areas.
The first area includes direct operating costs relating to each business unit; these are costs directly related to carrying out the priorities of the strategic plan and other ongoing mission-related programs. Two programs to be eliminated in FY15 are Partners for Progress (PfP) and Patient Management Perspectives in Otolaryngology (PMP). Also in FY15, the Washington, DC, office will be closed, although a small work space will be retained. In addition, the FY15 budget includes expenses related to expanding Quality Measures Development and added support to create a plan for the development of a comprehensive curriculum for otolaryngology.
The second area, allocated costs, relates to staffing and benefits as well as the operating costs that are incurred for the good of the whole organization, such as occupancy and building-related expenses, and organizational-wide HR, financial, and IT costs. Overall, allocated costs have increased due to inflation, contractual commitments, and salary adjustments; direct operating expenses have decreased due to the location of the 2014 Annual Meeting & OTO EXPOSM and streamlining other expenses.
The complete budget is available to any Academy member who requests it in writing. Email requests to Brenda S. Hargett, CPA, CAE, COO, to bulletin@entnet.org. James E. Saunders, MD
AAO-HNSF Coordinator
for International Affairs
International relations have long been an integral part of our Academy. The first international satellite and joint meeting with the Pan-American Otorhinolaryngology and Broncho-esophagology Congress was hosted in 1946 by the AmericanAcademy of Otolaryngology and Ophthalmology under the leadership of AAOO President Gordon New, MD, Chevalier Jackson, MD, and Paul Hollinger, MD.
Since then we have seen tremendous growth in the international scope of the AAO-HNS/F. Today nearly 40 percent of physician attendees at the Annual Meeting & OTO EXPOSM come from outside the United States. These attendees and our international members represent the best and the brightest of the global community of otolaryngology.
Our Academy is actively working to engage with these international colleagues. One cornerstone of this effort is Global Health 2014: Your Academy around the World. Originated by Gregory W. Randolph, MD, and now in its fourth year, this Miniseminar is a wonderful opportunity to hear international experts talk about their work and otolaryngology at home. At this exchange, we often find there are both striking similarities and differences in the problems we face.
Relatively new at the 2014 Annual Meeting is the International Assembly, in which Academy members and guests from our 55 International Corresponding Societies will honor the recipients of the International Visiting Scholarships and hear from our Academy leadership on topics of international interest.
The Academy is also proud to collaborate on five joint meetings with international societies throughout the year and four international satellite events at the Annual Meeting, including the new offerings of a Francophone Otolaryngology Update and a Combined AAO-HNSF and Middle Eastern Otolaryngology Societies Meeting Saturday, September 20 in Orlando.
As you can see, an important element of international relations is still getting otolaryngologists together in the same room. But, unlike that early meeting in 1946, we have new tools to help us reach out to otolaryngologists from around the world.
Last year, the Academy took the idea of a joint meeting one step further by reaching out to our Latin American Colleagues with a Latin American Webcast. More than 300 Latin American otolaryngologists participated in a Spanish-translated simulcast from Vancouver. This year we hope to expand this theme with an even wider distribution in Latin America and a broader international audience.
With the expansion of virtual meetings such as this, online journal access to Otolaryngology–Head and Neck Surgery, continued expansions in our online educational materials for international members, and online communities such as ENTConnect, your Academy keeps changing and evolving to maintain its position as a leader in the global community of otolaryngology.
Our Annual Meeting in 2014 promises to be the most advanced and internationally connected gatherings of otolaryngologists yet. Perhaps it is fitting that such a meeting should take place in Orlando, home of EPCOT®.
Just before his death, Walt Disney described his vision for the project as a “community of tomorrow” that will constantly change and never be completed. Today, the theme park is a “celebration of human achievement, technology innovation, and international culture.” Sounds a bit like our Academy, doesn’t it? Kavita Dedhia, MD
Humanitarian Travel Grantee
Raj C. Dedhia, MD
As husband and wife, we had the unique experience of traveling together from Pittsburgh, PA, to Butajira, Ethiopia, in early June to take part in a surgical mission for patients with chronic ear disease.
The trip was made possible by the collaboration of Ethiopian physician Nega Kiros, MD, and leader of Global ENT Outreach (GEO) Richard Wagner, MD. Dr. Wagner assembled an international team including himself, Marta Sandoval, MD (ENT-Spain), Pedro Benitez, MD (ENT-Spain), and Victor Estevez, MD, (Anesthesia-Spain) on the “Butajira Middle Ear Program.”
Dr. Wagner founded GEO in 2000. The organization has flourished during the last 13 years and now serves more than 10 countries. Dr. Wagner successfully established two temporal bone laboratories, one in Peru and the other in Cambodia.
Apart from the chief goal of providing patient care, there was a strong emphasis from the attending physicians on educating both Ethiopian otolaryngologists and us, residents from the United States. Two of the three microscopes had teaching arms allowing for attending oversight during cases. Additionally, one of the microscopes was hooked up to a projector system. This allowed the surgery to be viewed by a larger audience to allow better visualization of the procedures.
We met in Addis Ababa on Sunday, June 10, and traveled by car to the small town of Butajira. That afternoon, we evaluated nearly 100 pre-screened patients in clinic for surgical candidacy. While they patiently waited outside to see if they were to have surgery, we spent the next few hours triaging the group. We scheduled a total of 51 surgeries during the following five days.
We set out to complete roughly 10 complex cases per day including tympanoplasties, mastoidectomies, and tympanomastoidectomies with and without ossicular chain reconstruction. We used one large operating room, which was divided into three sections to maximize our efficiency by operating on up to three patients simultaneously. The majority of cases were performed under monitored anesthesia care (MAC) while younger children received general anesthesia.
Our day started with team breakfast at 7:30 am with an 8:00 am operating room start. We typically finished cases by 6:00 pm. Following dinner, we reviewed each of the cases from the day and reviewed surgery that had been recorded on one of the microscopes. It provided an excellent opportunity to reflect on our operative mistakes and learn from the experiences of others. Teaching the Ethiopian residents and physicians was the central goal of this surgical mission.
From June 11 through 15, we completed 51 otologic surgeries without notable complications. We provided care to an area that is profoundly underserved. To give perspective, the ENT nurse in Ethiopia stated that there were roughly 10,000 patients in Butajira on the waiting list to be seen in our clinic and possibly require surgery as sequelae from chronic otitis media. Ethiopia has a limited number of otolaryngologists, and of the otolaryngologists few are adept at providing complex otologic care. There are also virtually no supporting services such as trained audiologists and speech therapists. All of these factors increase the burden of ear disease in Ethiopia.
It is the hope of Dr. Wagner and the GEO to continue to train Ethiopian otolaryngologists (roughly 20 ENTs in a country of 84 million) in complex otologic surgery. In particular, the GEO is attempting to build an Ethiopian partnership to house a temporal bone laboratory in Addis Ababa and raise awareness for the devastating impact of middle ear disease.
We would like to thank the Academy for its generous support in providing Kavita the Humanitarian Travel Grant and allowing us the incredible opportunity to give back to the global community. Kanwar S. Kelley, MD, JD
Bryan Brandon, BS
Hamid Z. Djalilian, MD
For 200 years, the cause of Ludwig van Beethoven’s deafness has been the subject of much conjecture and intrigue. A great deal of controversy exists about Beethoven’s illnesses, of which there were many, and about the cause of his death. Many have tried to establish a unifying theory for his various illnesses, citing syphilis, Crohn’s, and lupus as potential diagnoses.1
What we do know is Beethoven exhibited diminished speech discrimination, hyperacusis, and progressive bilateral hearing loss (left greater than right), progressing to profound deafness during the course of his life, which was associated with constant bilateral tinnitus, but no vertigo.2
For the first time, we propose migraine-related hearing loss as a possible etiology of his deafness. There is evidence from various accounts that Beethoven suffered from chronic headaches, and it has been theorized that these headaches were migraine-related.3
Unfortunately, there is little literature documenting the exact nature of the headaches, but we do know Beethoven suffered from nearly all of the most common migraine triggers—poor sleep, irregular diet, and symptoms consistent with irritable bowel syndrome, which is frequently related to migraines.4,5
He was afflicted by recurrent colicky abdominal pain and alternating bouts of diarrhea and constipation, which have led many to believe he suffered from inflammatory bowel disease.6
In 1810, the same year as his last documented bout of headaches, he was described as having poor, “fitful” sleep, preferring wakefulness to any kind of sleep.4,5 In addition, Beethoven was noted to have a long history of depressive symptoms and myriad of life stressors.4
While the cause of Ludwig van Beethoven’s hearing loss will likely forever remain unknown, we propose adding migraine-related hearing loss to the long differential diagnosis.
References
Kubba A, Young M. Ludwig van Beethoven: a medical biography. Lancet. 1996;347:67-70.
Shearer PD. The deafness of Beethoven: an audiologic and medical overview. Am J Otol. 1990;11: 370-374.
Davies PJ. Beethoven in person: his deafness, illnesses, and death. Westport, CT: Greenwood Press; 2001.
François MM. Diagnosing genius: the life and death of Beethoven. Ithaca, NY: McGill-Queen’s University Press; 2007.
Albrecht T. Letters to Beethoven and other correspondence. Lincoln, NE: University ofNebraska Press; 1996.
Cooper M. Beethoven: the last decade. New York, NY: OxfordUniversity Press; 1985. In our ongoing efforts to address the results of the 2013 Education Needs Assessment Initiative, the Foundation will introduce enhancements to current education activities that are key drivers of engagement with the AAO-HNS/F. The Needs Survey measured the value of the Foundation Education Program on three levels: how a member rates the program on its own merits; in comparison to other organizations’ education activities; and on the likelihood to recommend to others.
The Education Steering Committee (ESC), comprised of the eight Education Committee chairs and under the leadership of Sonya Malekzadeh, MD, has reviewed all of the current education products offered by the Foundation based on the data gathered throughout the needs assessment. They developed a comprehensive list of enhancements to current activities and other changes that will increase the effectiveness of the Foundation’s education offerings.
Plans have been set to enhance existing education activities that have a strong influence on member engagement. A brief description of these enhancements follows.
AcademyQ®
Since its introduction in 2012, AcademyQ has seen immense growth and popularity. Those who have used the mobile app appreciate it for “offering a representative set of questions across all subspecialties” and “providing consistently high-quality content.” Knowing there is a need for constant updates in order to keep the app a useful product, the Foundation will add hundreds of new questions this year. Also exciting is the ability now to offer the app for operating systems other than Apple. This will allow the Foundation to build the new version of AcademyQ during the next several months.
Home Study Course
It’s probably no surprise to anyone that the Home Study Course (HSC) is most otolaryngologists’ first experience with the Foundation and a huge driver of member engagement with the Academy. Members report that it “provides consistently high-quality content” and “offers a reasonable price for the course.” HSC also succeeds in “covering the appropriate depth of content within each of the specialties.”
A Home Study Task force has been convened under the leadership of Brad W. Kesser, MD, and Richard V. Smith, MD, both members of the Education Steering Committee (ESC). This Task Force is charged with developing a plan to update and enhance the Home Study Course experience for a broader base of members. The Task Force conducted a survey with all current HSC subscribers. The survey yielded excellent information that will be used when developing a road map for the future of the activity. The Task Force plans to present its report to the ESC in September.
Annual Meeting & OTO EXPOSM Program Content
The Annual Meeting & OTO EXPOSM is also a strong driver of member engagement. About one-third of members attend the Annual Meeting every year while an additional 40 percent attend every few years. For those who attend the meeting, the part of the experience that has significant influence is “providing consistently high-quality content” and “offering an appropriate balance of clinical and practice management education.” Information from the education needs assessment has flowed into a comprehensive assessment of the annual meeting. One component of this assessment is to take a look at how Annual Meeting education content can be repurposed and offered to a wider member audience. Look for greater opportunities to access this content soon.
Clinical Otolaryngology Online (COOL)
COOL is designed for the non-otolaryngologist. For those who have used COOL, the resource influences their engagement in the education program. These individuals seek a resource that “provides an easy-to-understand assessment of otolaryngology-related topics” and “provides adequate information to make an appropriate otolaryngology referral.”
There is an increased emphasis at the Academy on reaching out to non-physician healthcare providers who work in otolaryngology-head and neck surgery. A re-evaluation and the development of new COOL courses is a part of this effort.
Coding and Reimbursement Workshops
Those respondents who have attended the Coding and Reimbursement Workshops indicate that their experience had a significant influence on their overall engagement with the Foundation.
Due to the timeliness and imperative regarding the adoption of ICD-10 in physician practices, the Coding and Reimbursement Workshops now has a third session on ICD-10 implementation. This full-day workshop assists both physicians and their staffs in preparing for the transition.
eBooks
It is very exciting to report that three AAO-HNSF publications are being updated and re-released in the next 12 months. Because of a formal publishing agreement the Foundation has entered into with Thieme Publishing, two books will be published online and in print this year. Geriatric Care Otolaryngology is being updated under the leadership of Robert T. Sataloff, MD. Otolaryngology Lifelong Learning Manual, a revised version of the Maintenance Manual for Lifelong Learning, will also be published under the leadership of Sonya Malekzadeh, MD, and the Education Steering Committee. Members of the eight Education Committees served as chapter reviewers and authors.
The Quick Reference Guide to Neck Dissection Classification and TNM Staging of Head and Neck Cancer is also being revised under the leadership of Daniel B. Deschler, MD. This will be the fourth edition of this helpful resource that will include the most recent AJCC Cancer Staging Tables.
Online Education
Online Education including the Online Lecture Series (OLS), which are recordings of Annual Meeting Instruction Courses and Online Courses that are developed by Education Committee members contribute influence by “presenting content logically so that it is easy to follow,” “providing consistently high-quality content,” and “covering the appropriate breadth of content across specialties.”
A clear message from the Needs Assessment Survey was the strong recommendation that the Foundation education activities be more web-based and more engaging. Look for new online courses that are cased-based, interactive, and self-paced.
A new Learning Management System will be built that will offer many more opportunities to develop high quality and engaging activities. In addition, the Professional Development pages of the new entnet.org have been redesigned to provide access to the resources members need to engage in education with the Foundation. Continue to look for improvements to current popular education products and the introduction of new eLearning technology to enhance relevance to members. What to Do Now to Mitigate Financial Risk
Cheryl L. Toth, MBA
Practices have many competing, high priorities these days: dealing with Electronic Health Records (EHR) implementation, qualifying for Meaningful Use, conducting diligence on the hospital’s employment offer, and, of course, transitioning to ICD-10.
Right now, everyone in the office is (rightfully so) running around, cross walking codes, modifying dictation habits, and chasing down payer end-to-end testing dates.
Meanwhile, back in the billing office, attention is slowly slipping away from the accounts receivable. Following up on overdue insurance balances, setting up patient payment plans, monitoring the A/R as they typically would are taking a back seat to ICD-10 and other “distractions.” This should concern you. A lot.
Despite competing priorities, practices must take the time to plan ahead for a potential post-October 1, 2015 revenue hit. Ripped from the headlines, here’s why:
“Implementation of ICD-10 May Cause Serious Cash Flow Problems for Providers.”1
This is according to many sources—most notably the Department of Health & Human Services (HHS). Enough said.
If you don’t already have one, apply for a line of credit soon. Banks prefer to dole these out before they are actually needed. And come October 2015, you don’t want to be the 45th physician in line at the bank, pleading for help.
You’ll rely on a line of credit less if you’ve got some cash squirreled away, so build a nest egg this spring and summer. Focus on cleaning up 90-day and 120-day insurance receivables—which typically have the highest payoff for the least effort. Hiring an experienced biller or collections specialist to conduct this cleanup on a project basis is money well spent. Having an extra set of hands frees up the billing team for transition planning and testing, as well as the potential deluge of claim denials and technology glitches after. Ask for a summary of follow-up results monthly. Set a goal to have the insurance A/R cleaned to the point that no more than 10 percent of all payer receivables are less than 90 days old on September 30 of next year.
For past due patient accounts, launch a “spring collection campaign.” Seventy-four percent of patients said they were willing and able to pay out-of-pocket expenses less than or equal to $1,000, and 62 percent were willing to pay medical bills greater than or equal to $1,000. Thirty-seven percent of patients said that a lack of payment options was the reason they didn’t pay healthcare bills.2 Interpretation: Do a better job asking patients to pay, and give them more payment options.
Instruct staff to focus on the highest balances first, and work accounts in descending balance order—not alphabetical order. Offer online bill pay through your vendor’s patient portal or a company such as TransFirst (www.transfirst.com) or PayPal (www.paypal.com). And make budget plan setting simple by offering patients automatic recurring payments. Like a Netflix subscription or gym membership, such payments are automatically charged to the patient’s credit card each month. TransFirst or PayPal also offer this feature.
“A Fifty Percent Decline in Productivity” and “Expect that Staff Will Have to Spend More Time in Follow-up with Plans.”
In its ICD-10 Implementation Guide for Small Practices, the Centers for Medicare & Medicaid Services (CMS) warns practices to expect more claim denials and an increased follow up time.3 Multiple reputable sources and studies predict significant slowdowns in staff’s ability to code a claim or case and get a claim out the door. ICD-10 pilot results presented at the Medical Group Management Association (MGMA) 2013 annual conference mirrored the experience of Canada’s ICD-10 transition: staff productivity drops 50 percent when staff attempted to identify the proper ICD-10 codes from physician documentation.4,5
Don’t deny these productivity predictions, and don’t wait until next summer to hire people. Staff up now, before the hospital snaps up the best candidates.
And if you think outsourcing the billing is a solution—it’s not. Even under the best circumstances, the outsourcing process is painful. And what if the billing company isn’t fully prepared for ICD-10? Better to hire an additional part-time or full-time coder and/or billing office staffer capable of consistent denial management who will keep cash flowing come fall.
“Docs Charting Falls Short of ICD-10 Demands.”6
While this information is not a complete surprise, it should be an eye opener for those who were hoping “someone in billing” would handle ICD-10, instead of the physicians. Actually, nothing could be further from the truth. Without the additional detail required by ICD-10, coders won’t be able to select the right code, resulting in backlogs of claims (read: unrealized revenue) and the need for staff to constantly follow up with physicians to obtain more detail.
And don’t forget about prior authorization letters for surgeries after October 1, 2015, which must be written to justify medical necessity using ICD-10 terms and codes. Because prior authorizations are typically done three to four weeks before surgery, physicians will be pre-authorizing in ICD-10 at least three or four weeks ahead of the deadline. If surgeries are booked months in advance, your practice may be required to pre-authorize (and pre-certify) using ICD-10 as early as next summer.
Revise dictation prompters and letter templates and check payer sites to determine how date of service and date of discharge affect which system to use for procedures scheduled close to October 1.
For other ICD-10 resources, visit the Academy’s ICD-10 page at http://www.entnet.org/Practice/International-Classification-of-Diseases-ICD.cfm.
Cheryl Toth, MBA, is a senior consultant and writer with Karen Zupko & Associates, Inc.
Please note: After passage of Protecting Access to Medicare Act of 2014 (PAMA) the deadline for compliance is now October 1, 2015.
References
1. Seidman M. ICD-10 and Version 5010. Bulletin. April 2012;31(4):11. http://bulletin.entnet.org/Assets/AAOBulletin/pdf/Bulletin_Apr_2012.pdf
2. McKinsey & Company. McKinsey on Payments. April 2009. http://www.mckinsey.com/App_Media/Reports/Financial_Services/US_healthcare_payments_Remedies_for_an_ailing_system.pdf
3. ICD-10 Implementation Guide for Small and Medium Practices. Issue brief. Centers for Medicaid Services 2013. Web. 1 Aug. 2013. http://www.cms.gov/Medicare/Coding/ICD10/Downloads/ICD10SmallMediumPracticeHandbook.pdf
4. McCann E. The ICD-10 Pilot That Was Just Plain ‘Scary.’ Government HealthIT. October 14, 2013 http://www.govhealthit.com/news/icd-10-pilot-was-just-plain-scary-coding-coders
5. Implementing ICD-10: A Canadian Perspective from the Front Line. Revenue Cycle Strategist. 2009:3. http://www.hfma.org/Publications/Newsletters/Revenue-Cycle-Strategist/Archives/2009/February/Revenue-Cycle-Strategist—February-2009-Issue/.
6. Pittman D. Docs Charting Falls Short of ICD-10 Demands. MedPage Today. April 12, 2013.
Learn More
Learn more revenue-cycle tactics and technologies at the Academy-sponsored workshop Kicking Revenue into High Gear.
Attend an AAO-HNS Coding & Reimbursement workshop as soon as possible. Physicians should be practicing in ICD-10 regularly.
Visit http://www.entnet.org/coding.