More from March 2014 - Vol. 33 No. 03

In 1946, thanks to the vision and leadership of Chevalier Jackson, MD, with U.S. and Latin American colleagues, the Pan-American Association of Oto-Rhinolaryngology-Head and Neck Surgery was founded in Chicago, IL, during the 51st meeting of the American Academy of Otolaryngology—Head and Neck Surgery.
Responding to the need for a strong scientific and social exchange among specialists on our continent, the Association has created the great and enduring Pan-American community that has organized the Pan-American Congress of Otolaryngology continuously every two years for more than six decades.
All members of accredited societies of otorhinolaryngology in the Americas—including Academy members—are active members of the Pan-American Association.
As president of the XXXIV Pan-American Congress, it is an honor and privilege to extend a special invitation to all Academy members to join us
October 26-29 in the beautiful city of Cartagena, declared a World Heritage Site by UNESCO in 1984.
Roy R. Casiano, MD, of the University of Miami, immediate past president of the Panamerican Association and past chair of the Academy’s Panamerican Committee stated:
“Attendees will be exposed to the latest scientific and technological advances within the various disciplines of otolaryngology, while enjoying the warm camaraderie that our social events bring.”
President of the Pan-American Association Luis A. Macias, MD, of Mexico City, expressed:
“One of the statutory principles of our Association is the exchange of knowledge and advances in our specialty for the benefit of our patients; this task has been fully complied in our meetings, thanks to the active participation of its members.”
Undoubtedly, Cartagena is a Colombian touristic and historic jewel of the Caribbean—it has hosted the most important world events of politics, science, and international trade. Cartagena has a world-class hotel infrastructure and the Las Américas Global Resort and InternationalConvention Center meet all the criteria for a successful Congress.
A highlight of the Congress program will be a joint meeting of the Academy and the Panamerican Association, supported by James E. Saunders, MD, international coordinator, and J. Pablo Stolovitzky, MD, regional advisor for Latin America, with speakers from both societies. In addition, the Congress will provide a booth for the Academy to display its educational offerings in the exhibit hall.
I specially recommend our Pan-American Association website (http://www.panamorl.com.ar/) excellently managed by Hector E. Ruiz, MD, of Rosario, Argentina, founder and past chair of the AAO-HNSF Panamerican Committee.
On behalf of the Colombian Society of Otolaryngology, our president, Antonio Jose Reyes Solarte, MD, our scientific coordinator, Roxana Cobo Sefair, MD, the organizing committee, and all Colombian otolaryngologists, we hereby extend a friendly invitation to all Academy members.
For details, visit www.panamorl2014.com.
Key Dates to Remember
Early bird registration is open until March 31.
Scientific Program abstracts submissions deadline is June 30. Audrey P. Calzada, MD
Clinical Fellow, Otology/Neurotology
House Ear Clinic
I had the privilege of traveling as part of the team led by Glenn Isaacson, MD, with Healing the Children to Ethiopia at the end of October. We spent two days in Addis Ababa giving lectures to the otolaryngology residents at Addis AbabaUniversity and seeing mostly children in a clinic at the mission hospital, CURE, and at the MakanissaSchool for the Deaf. We spent the remainder of the week in Mekelle, the third largest city in Ethiopia. We operated on and saw patients with Adamu Yilikal, MD, who is the only otolaryngologist in the northern half of the country, serving more than eight million people. The goal of our trip was to equip local surgeons to better serve their communities by providing equipment, clinical instruction, and operative teaching.
Our team consisted of four otolaryngologists, one anesthesiologist, three audiologists, and the president of Healing the Children. We had the opportunity to provide and observe medical care in several different healthcare settings within Ethiopia: a non-profit mission hospital, a government hospital, and a mission school for the deaf. Visiting and working in each center allowed for comparing and contrasting the benefits and downfalls of each place in partnering to provide healthcare to the people of Ethiopia.
We began our week at the mission hospital, CURE, which is a non-profit, privately funded surgical hospital for children in Addis Ababa with high standards of excellence. Because Dr. Isaacson and anesthesiologist Elizabeth Drum, MD, have led multiple teams there during the past five years, the clinic we ran consisted of both new and returning patients, who had previous operations by our team. The equipment, all donated and brought by surgical teams, was organized and sufficient. The flow of the operating room, directed by an anesthesiologist from the United States, was efficient and smooth. While this surgical hospital provides excellent, free care to children, the leadership is largely foreign-based and western-trained, which limits its ability to build local healthcare expertise.
In contrast to CURE, the government hospital in Mekelle, where we performed otologic and head and neck cases with Dr. Yilikal, was poorly equipped and inefficiently run despite hard-working, intelligent staff. One main hindrance to safe operative care in Ethiopia is the absence of anesthesiologists with medical degrees. In addition to training Dr. Yilikal and his residents to perform essential otolaryngologic procedures, we provided surgical instruments and equipment. Despite working there for two years and being the only otolaryngologist in the region, he had instruments to perform only tonsillectomies prior to our visit. In addition to the lack of well-trained ancillary staff and equipment, there was also the issue of consistent electricity in this large government hospital. It was extremely humbling to realize the large amount of infrastructure required to perform safe operations.
The Ethiopian leaders of the government hospital in Mekelle were overwhelmingly hospitable. Through discussions with them over meals in the evening, I was inspired by their simultaneous understanding of the plight of medical care in Ethiopia and their courage to continue seeking out opportunities to improve the standard of care. I began to better understand the issues developing countries face when their educated class chooses to live and work in other countries with more opportunities. Even if disregarding financial provision for their families and future educational opportunities for their children, there is a seemingly insurmountable ceiling of advancement within surgical subspecialties. Not only are opportunities to develop adequate surgical skills in quality training programs lacking, there is no support or equipment to build a meaningful practice. What impact can a practicing otolaryngologist in a community of eight million people make without a microscope, surgical instruments, and trustworthy anesthesia?
These are issues that have been courageously and tirelessly addressed by Dr. Isaacson (Dr. Glenn, as he is known in Ethiopia) during the past six years. To detail the equipment and support provided to the Ethiopian otolaryngology community is one thing, but I was equally struck by his tenacity in dealing with the minute-to-minute issues we all faced with improvisation and patience. As my emotions regarding medical humanitarian work positively impacting a developing community wavered between hopelessness and optimism, I observed that our trip leaders were quietly and diligently changing the practice of otolaryngology in Ethiopia.
As I complete my fellowship training, I desire to be useful in service to others, and I hope to partner with surgeons in other parts of the world to better serve their communities. I am thankful to the AAO-HNSF Humanitarian Committee for providing grant support for this trip. I return inspired and humbled by the attitudes and hard work of my colleagues both in this country and in Ethiopia. Ahmed M. S. Soliman, MD
Five years since its conception and after nearly a year of planning, the first Combined Satellite Meeting of the American Academy of Otolaryngology—Head and Neck Surgery and the Egyptian Society of Otorhinolaryngology took place September 28, 2013, in Vancouver, BC, Canada.
This historic event was co-chaired by Ahmed M. S. Soliman, MD, of Temple University and Prof. M. Adel Khalifa, MD, of Tanta University, Egypt. Eugene N. Myers, MD, FRCS Ed (Hon), professor and chair emeritus, University of Pittsburgh, and Prof. A. Sameh Farid, MD, dean of the CairoUniversityMedicalSchool, presided over the conference, which included presentations by members of both organizations. Prof. Khalifa presented Dr. Myers with the Honorary Shield of the Egyptian ORL Society for his many contributions to advancing cooperation between the two groups.
James L. Netterville, MD, president of the AAO-HNS, and President-Elect Richard W. Waguespack, MD, gave welcome remarks. Scientific presentations included “Endoscopic Management of Reinke’s Edema” by Peak Woo, MD, “Treatment of laryngeal malignancies with plasmonic photothermal therapy” by Prof. Hazem Saleh, MD, and “Correlation between neural response telemetry and CT scanning of electrode position in pediatric cochlear implant patients” by Ahmed H. Allam, MD.
Other presenters included G. Richard Holt, MD, D-BE, MSE, MPH; Ivan H. El-Sayed, MD; Ellen S. Deutsch, MD; Nicholas Y. BuSaba, MD; Gregory W. Randolph, MD; Basim M. Wahba, MD, DOHNS, MRCS; and Prof. Ahmad S. El-Guindy, MD.
The meeting concluded with a dinner reception at Milestones Vancouver. Drs. Allam and Wahba, 2014 AAO-HNSF International Visiting Scholars, were honored at the International Assembly and International Reception.
Two previous combined meetings of the two societies, in 2012 and 2013, planned for Cairo, had been cancelled because of political unrest. In his closing remarks, Dr. Randolph, chair, International Steering Committee, congratulated the organizers for their persistence and perseverance that finally brought the meeting to fruition despite many odds. The future of continuing medical education (CME) will be based on the latest technology available. Increasingly, physicians are seeking online resources to get CME credit. This trend is likely to continue as the time constraints of a busy practice will require you to seek easily accessible professional development opportunities.
Physicians are becoming increasingly technology savvy. Recent studies have shown a general shift to physicians preferring online CME activities. The trend is also more mobile with the majority of physicians owning smartphones and tablets. Many use these tools to search for and download clinical information. Many see the trend toward increased virtual CME and are embracing it as a viable alternative to live activities.
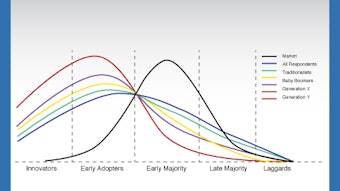
Otolaryngologist-head and neck surgeons are no exception to the tech savvy trend. According to the recent Member Education Needs Survey, the majority of members consider themselves innovators or early adopters of technology, including online learning, e-books, and mobile applications. There was a clear preference among members for more Web-based education formats.
Members indicated they are using smartphones, tablets, and e-readers for continuing education information. According to the survey, 55 percent use a tablet, 54 percent use a smartphone, and 13 percent use an e-reader as a source for both continuing education and professional information. Preferred learning formats included online self-paced courses, smartphone and tablet apps, and webinars.
When asked what changes are expected that will affect their education needs, many member responses centered on new e-learning technology. These include an increase in:
The move to online learning
Virtual meetings and lectures
Materials available on smartphones and tablets
Online material supplanting print methods
Interactive, online content and assessment
Easily available e-seminars
Faster and more up-to-date information available on the Web
Internet-based teaching
Online asynchronous learning
Simulation
The Foundation is continually exploring ways to improve education opportunities for members. New technologies within professional education provide many options to enhance one’s learning experience. Survey respondents offered useful suggestions about integrating more technology into the Foundation’s education program. Because of these preferences and expectations, the focus will be toward more e-learning in the design of future education and knowledge resources.
There are several projects in the works at the AAO-HNS/F that, through technology, will provide more meaningful and rewarding education, knowledge products, and services for you in 2014.
Your feedback indicates that in addition to traditional educational methods, a growing number of members desire a larger e-learning environment and expanded electronic platform.
Armed with a better appreciation of our members’ preferred learning styles in education and training, combined with today’s expanding technology, we will be better equipped to offer many new and varied formats to enhance learning experiences. Background
Under the Affordable Care Act (ACA), the Centers for Medicaid & Medicare Services (CMS) is required to develop a Physician Compare website with information on physicians enrolled in the Medicare program, and information on other Eligible Professionals (EPs) who participate in PQRS. Essentially, CMS is charged with making information on physician performance, including information on quality measures and patient experience, available through the Physician Compare website. To meet that end, CMS must send a report to Congress on Physician Compare development, including information on efforts and plans to collect and publish data on physician quality and efficiency, and on patient experience of care in support of value-based purchasing and consumer choice by January 1, 2015. The ACA allows for CMS to expand information made available on Physician Compare any time before that date.
The first phase of the website launched in 2010, but in 2013, CMS released a redesigned Physician Compare website. The primary source of administrative information on Physician Compare is from the Provider Enrollment, Chain, and Ownership System (PECOS), with the use of Medicare claims information to verify the information in PECOS. It is important to note that members must ensure their information is up-to-date and accurate in the national PECOS database. In addition, any information not found in PECOS, such as hospital affiliation and foreign language, must be updated by emailing the Physician Compare team at physiciancompare@westat.com.
Information that is currently reflected on the site includes: address; education; American Board of Medical Specialties (ABMS) board certification information; primary and secondary specialties; group affiliations; hospital affiliations that link to the hospital’s profile on Hospital Compare as available; Medicare Assignment status; and Provider language skills.
In addition to the aforementioned, the Physician Compare website also includes:
Individual Quality Information
On each individual profile page there is a section listing the quality programs under which the specific individual satisfactorily reports and if he or she is a successful electronic prescriber. A notation and check mark for individuals that successfully participate in the Electronic Health Records (EHR) Incentive Program is also included.
Group Quality Information
In addition to that included for individuals, CMS also built-in a quality programs section for each group practice profile page to indicate which group practices are satisfactorily reporting using the GPRO web-interface for PQRS reporting, or are successful electronic prescribers under the eRx Incentive Program.
New Additions to Physician Compare
Within the newly released CY 2014 Medicare Physician Fee Schedule Final Rule, several new additions to the Physician Compare website were finalized. These changes include the following:
Physician Compare will publicly report ALL quality measures collected through the Group Practice Reporting Option (GPRO) web interface for groups of all sizes. Note: A 30-day review period for quality measures on Physician Compare will be given, but not for non-measure data such as telephone number, specialty, etc.
Physician Compare will publicly report performance on GPRO registry and EHR measures. Note: CMS highlighted that it will conduct analyses to ensure that measures collected via different mechanisms are consistently understood and only measures proven to be comparable and most suitable for public reporting will be included on Physician Compare.
Physician Compare will publicly report Clinician and Group Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) measures for groups of 100 or more EPs who participate in PQRS GPRO, regardless of submission method.
Physician Compare will publicly report CG-CAHPS for Medicare Shared Savings Plan (MSSP) Accountable Care Organizations (ACOs) reporting through the GPRO web interface.
Physician Compare will publicly report CG-CAHPS measures collected via a certified CAHPS vendor for groups of 25 to 99 EPs.
Physician Compare will publicly report performance on 20 measures listed in the proposed rule that are reported by individual eligible professionals reporting through an EHR, registry, or claims during 2014 under the PQRS. Note: The only measures that appear applicable to ENTs for the above categories are Medication Reconciliation and Preventive Care and Screening: Tobacco Use: Screening and Cessation.
CMS plans to publicly report 2014 data in CY 2015. For more information on Physician Compare, visit www.medicare.gov/physiciancompare or email the health policy team at healthpolicy@entnet.org. Rahul K. Shah, MD
George Washington University School of Medicine, Children’s National Medical Center, Washington, DC
The concept of value in healthcare is not novel—almost everyone is familiar with the well-known equation: value = quality of care/cost of such care. To increase the value of healthcare delivery, we can simplistically increase the quality of the care that is delivered or the perception of that delivered care; one can also reduce the cost of that care.
Currently, the in-vogue statement is “value-based purchasing.” This month’s column will attempt to convey my strong sentiment about how value-based purchasing is actually a complex transaction that will fundamentally change the way we approach the care we deliver to patients. Further, Academy members are uniquely positioned, as a result of the diverse patients we care for, to lead and help explain this concept within our offices and organizations.
The concept of value-based purchasing is predicated on the premise that with all else being equal, the cheaper option should be chosen. Using the value equation above, we can see that if we hold the quality of care as a constant, then the way to drive up the value of care is to choose the less costly alternative. Value-based purchasing is juxtaposed to volume and intensity of service programs.
Healthcare has been predominantly based on the volume/intensity of service model. For example, more cases generate more volume, which means the “rainmaker” would be more highly compensated; another way to think about volume-based reimbursement is that the patient that has a longer length of stay would yield more revenue to the hospital than a similar diagnosis patient that has half as long of a stay. Indeed, many hospitals are caught with feet in both of these worlds: the volume model and the value-based purchasing model.
I have been struggling to make the business case for quality from a surgical perspective within a paradigm of value-based purchasing. However, the following analogy should shed some light on this complex issue. Let us start with a common surgery that has more or less a relatively tight range of fixed costs to perform the case—an adenotonsillectomy. There are myriad techniques to perform this procedure, and they all have fixed costs that probably range from .5x all the way to about 4x (“x” denotes the average fixed costs to perform an adenotonsillectomy). We rarely think past this point, and I am sure that most Academy members are not too terribly concerned about the fixed costs of our cases.
However, in a value-based purchasing mindset, we would need to take into account the entire spectrum of care to make a business case. For example, if there is a method to perform an adenotonsillectomy that costs 4x (four times the average cost), then in a volume/intensity of care model, we may not look favorably at this method, and management/administration may not want this technique with such high fixed costs and low profit margins.
In an era of value-based purchasing, if the overall quality of the patient care improves and their outcomes improve, then there would be a rationale to consider using this device despite the increased fixed costs. For example, if the patient can be discharged sooner (even from PACU), the result is less use of hospital resources (expenses) and thus using the value equation from the opening of this column, the overall costs have decreased slightly but the quality for the patient has improved. This would result in higher reimbursement than otherwise in a value-based reimbursement model.
By using a concrete example from our realm of care, I hope this column helps explain how complex value-based purchasing/reimbursement is and how as healthcare providers we must be cognizant of the entire spectrum of the patient’s care delivery. This is even more complex for our Academy members as otolaryngology-head and neck surgery spans a uniquely broad (out-patient, in-patient, emergency, elective, etc.) range of care.
We encourage members to write us with any topic of interest and we will try to research and discuss the issue. Members’ names are published only after they have been contacted directly by Academy staff and have given consent to use their names. Please email the Academy at qualityimprovement@entnet.org to engage us in a patient safety and quality discussion that is pertinent to your practice. Last August, the Academy received inquiries from members who pointed out that the existing Correct Coding Initiative (CCI) edits for (non-endoscopic) CPT 31000 Lavage by cannulation; maxillary sinus (antrum puncture or natural ostium, permitted providers to circumvent the CCI edit of “1,” which bundles this service when performed in conjunction with codes 31256 Nasal/sinus endoscopy, surgical, with maxillary antrostomy and 31267 Nasal/sinus endoscopy, surgical, with maxillary antrostomy; with removal of tissue from maxillary sinus, by appending a -59 modifier. In response, we drafted a letter to the National Correct Coding Initiative (NCCI) staff and Centers for Medicare & Medicaid Services (CMS), noting that there are real, but uncommon, instances for which the modifier is appropriate, so the edit for these code combinations should not be “0.” We also noted that no CCI edit currently exists for the code combination of 31000 and 31295 Nasal/sinus endoscopy, surgical; with dilation of maxillary sinus ostium (e.g., balloon dilation), transnasal or via canine fossa.
NCCI staff responded that they, and accordingly, CMS agreed with the Academy that CPT 31000 may be reported separately with 31256 or 31267 if the lavage is performed on the contralateral sinus and may be reported with modifier 59 in such circumstances. CMS also agreed that it would be appropriate to add an edit bundling CPT 31000 into 31295, and that similar edits bundling 31000 and 31002 Lavage by cannulation; sphenoid sinus into other procedures of the maxillary and sphenoid sinuses respectively, based on the same rationale (i.e., lavage is integral to the more extensive sinus procedure). However, if lavage of a sinus and a more extensive procedure are performed on the contralateral sinus, they may be reported together with the appropriate modifiers.
These new edits will take effect April 1. For more information regarding this CCI edit change and proper coding for these services, visit our Coding Corner on the Academy website, which includes a CPT for ENT that outlines these issues further: http://bit.ly/CPT4ENT.
The Academy is pleased that CMS, and the NCCI, have agreed to implement this change. To access the full response from NCCI, visit http://bit.ly/NCCIMUE. We encourage members to keep health policy staff abreast of any similar coding issues they encounter in the future. We urge you to email us at healthpolicy@entnet.org with any questions related to this issue or other coding and reimbursement matters. OPPS 2014 Final Payment Rates
For Calendar Year (CY) 2014, CMS finalizes a hospital outpatient department conversion factor of $71.219. This is based on a hospital inpatient market basket rate increase of 2.5 percent, minus the proposed multifactor productivity (MFP) adjustment of -.5 percent, and the -.3 percent adjustment, which are both required under the Affordable Care Act (ACA). CMS has also proposed to continue implementing the statutory 2 percent reduction in payments for hospitals that fail to meet the hospital outpatient quality reporting (OQR) requirements.
Updates Affecting OPPS Payments
In CY 2014, CMS has continued the changes made in 2013 to base the relative weights on geometric mean costs rather than previously utilized median costs. It will continue to use these weights to set a cost to charge ratio within an APC to determine payment for services within an APC. In CY 2014, CMS finalizes several significant changes to their methodology to calculate APC payments, including:
Greatly expanding the types of services that are packaged and not paid separately;
Replacing the current five levels of visit codes for clinic visits with a single new alphanumeric Level II HCPCS code representing one level of payment for all clinic visits; the final rule maintains current codes for Type A emergency department (ED) and Type B ED visits;
Using distinct cost-to-charge ratios (CCRs) for cardiac catheterization, CT scan, and MRI to calculate the relative payment weights; and
Effective January 1, 2015, establishing comprehensive APCs for 29 device-dependent services and make a single payment for the comprehensive service based on all OPPS-payable charges on the claim.
To see a complete list of APCs and the influence on their payment rates, see Addendum B: http://www.entnet.org/Practice/loader.cfm?csModule=security/getfile&pageid=180429
Changes to APC Assignments Affecting Head and Neck Surgery
Within the final rule, CMS makes several changes to APC assignments for otolaryngology services, including assigning new CPT code 64617 Chemodenervation of Larynx to APC 0206 with a 2014 APC payment rate of $353.99. Further, CMS modifies the APC assignment of CPT 31571 Direct Laryngoscopy from APC 0075 to 0074, representing a change in reimbursement from $2,026.82 in 2013 to $1,880.43 in 2014. Similarly, CMS modified APC assignments for Balloon Sinus Codes CPT 31295 and 31296 to assign them to APC 0075 in CY 2014 and for 31297 and 31541 from APC 0075 to 0074 for 2014. This results in a change in payment for 31295 and 31296 from $2,026.82 in 2013 to $3,051.76 in 2014 and from $2,026.82 in 2013 for CPT 31297 and 31541 to $1,880.43 in CY 2014.
OPPS Payment for Hospital Outpatient Visits
For CY 2014, CMS establishes a single visit code for hospital clinics, replacing the five visit levels used in the OPPS since 2007. The mid-level clinic visit, APC 606, has been the most frequently used outpatient hospital visit code. Under the final rule, the new single level clinic visit, APC 0634, would have a base payment rate of $92.53 in 2014, a reduction of about 4.6 percent compared to the current payment rate of $96.96 for the mid-level clinic visit (APC 606). They believe a policy that recognizes a single visit level for clinic visits under the OPPS is appropriate for several reasons, including:
The policy is in line with their goal of using larger payment bundles to maximize hospitals’ incentives to provide care in the most efficient manner.
The policy will remove any incentives hospitals may have to provide medically unnecessary services or expend additional, unnecessary resources to achieve a higher level of visit payment under the OPPS.
The policy will reduce hospitals’ administrative burden by eliminating the need for them to develop and apply their own internal guidelines to differentiate among five levels of resource use for every clinic visit they provide, and by eliminating the need to distinguish between new and established patients.
Lastly, they believe that removing the differentiation among five levels of intensity for each visit will eliminate any incentive for hospitals to “upcode” patients whose visits do not fall clearly into one category or another.
Supervision of Outpatient Therapeutic Services in CAHs and Small Rural Hospitals
CMS ends its non-enforcement policy requiring direct supervision of outpatient therapeutic services in CAHs and small rural hospitals; thus, for years beginning with 2014, CAHs and small rural hospitals have to comply with the CMS supervision policy which requires direct supervision of therapeutic services, except for those that CMS identifies as appropriate for general supervision. CMS believes that it is appropriate to let this grace period expire to ensure the quality and safety of hospital and CAH outpatient therapeutic services provided by Medicare.
Supervision for Observation Services
In addition, CMS clarified that for observation services, if the supervising physician or appropriate non-physician practitioner determines and documents in the medical record that the beneficiary is stable and may be transitioned to general supervision, general supervision may be furnished for the duration of the service. Medicare does not require an additional initiation period(s) of direct supervision during the service. CMS believes that this clarification will assist hospitals in furnishing the required supervision of observation services without undue burden on their staff.
Hospital Outpatient Quality Reporting (OQR) Program
As established in previous rules, hospitals will continue to face a 2 percent reduction to their OPD fee schedule update for failure to report on quality measures in the OQR Program in CY 2014. Program measures can be accessed at www.QualityNet.org. In its final rule, CMS reiterates its intention that the hospital OQR program will transition to the use of certified EHR technology for submission of data on those measures that require information from the clinical record. CMS estimates this transition will occur sometime after 2015, and notes much work remains to reach this point, including developing electronic specifications, pilot testing, reliability and validity testing, etc.
ASC 2014 Final Payment Rates:
For CY 2014, the ASC conversion factor will increase 1.2 percent—this reflects the updated consumer price index (CPI-U) (a consumer price index for all urban consumers) of 1.7 percent, minus the projected multifactor productivity adjustment of -0.5 percent required by the ACA, and results in a proposed increase in the conversion factor from $42.917 in 2013 to $43.471 in 2014.
New ASC Covered Surgical Procedures for 2014
CMS approves four new procedures for coverage in the ASC setting in CY 2014. Notably, two of these procedures are commonly performed by ENTs: CPT 60240 thyroidectomy, total or complete and 60500 Parathyroidectomy or exploration of parathyroid(s). Both codes were assigned an ASC payment indicator of G2, meaning: Non office-based surgical procedure added to ASC list in CY 2008 or later; payment based on OPPS relative payment weight. CMS also flags new CPT code 64617 Chemodenervation of larynx as temporarily office-based for CY 2014 and assigns it a payment indicator of P3, meaning the payment rate is capped at the MPFS practice expense rate.
Surgical Procedures Designated as Office-Based
Annually, CMS proposes to update payments for office-based procedures and device-intensive procedures using its previously established methodology. Office-based procedures are defined as surgical procedures, which are used more than 50 percent in the physicians’ offices. For CY 2014, CMS permanently identified three additional procedures as office-based and has reviewed information for the eight procedures finalized for temporary office-based status last year. None of the services discussed relate to our specialty. The Academy, however, continues to track policy change in this area as several ENT services were added to this list in 2013 rulemaking.
ASC Quality Reporting Program:
In 2012, CMS finalized the implementation of an ASC quality-reporting program (ASCQR), which will begin with 2014 payment determination. Quality measures have been adopted for the calendar years 2014-2016. Payment penalties for ASCs who do not adequately report will remain at 2 percent. Penalties will be applied in CY 2016 payments based on 2014 reporting. Quality measures can be found at www.Qualitynet.org.
For more information on the final rule access the Academy’s full summaries of OPPS and ASC finalized requirements at http://www.entnet.org/Practice/Summaries-of-Regulations-and-Comment-Letters.cfm#CMSRegs or email questions to Academy health policy staff at HealthPolicy@entnet.org.